Medical Coding for Lacerations: ICD-10-CM, CPT, Documentation, and Billing Guidelines for 2026
By Janine Mothershed CPC, CPC-I
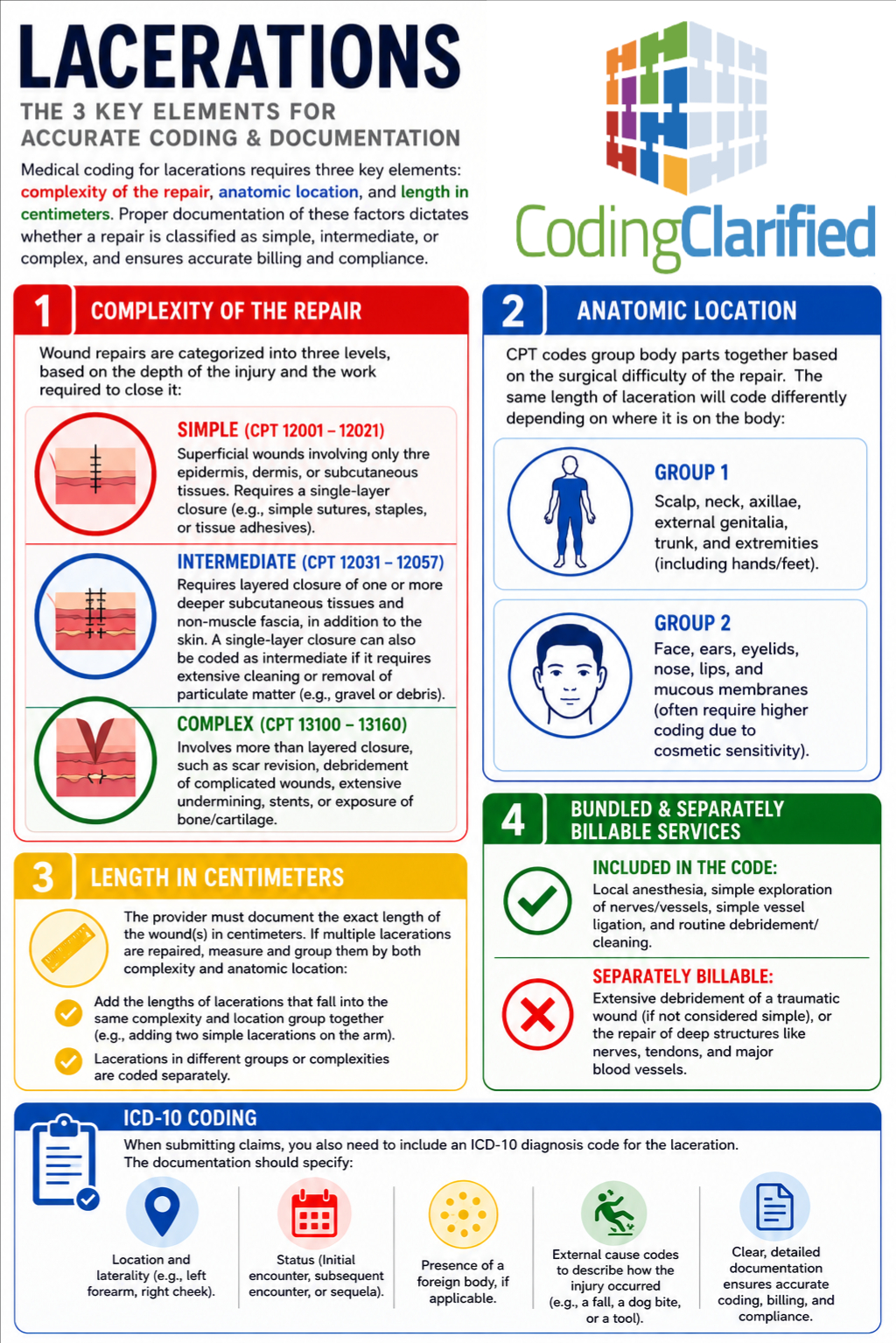
Laceration repair coding remains one of the most frequently reported services in urgent care centers, emergency departments, physician offices, and outpatient facilities. However, despite its common occurrence, laceration coding continues to generate coding errors, modifier issues, and claim denials.
Therefore, understanding how to correctly assign ICD-10-CM diagnosis codes, CPT repair codes, modifiers, and supporting documentation is essential for accurate reimbursement and compliance in 2026.
Whether you are a new medical coder, CPC student, physician, or experienced coding professional, this guide explains the latest best practices for coding lacerations.
Key Takeaways
- Laceration diagnosis coding begins with identifying the anatomical location, laterality, encounter type, and presence of a foreign body.
- CPT laceration repair codes are selected based on repair complexity and total wound length.
- Simple, intermediate, and complex repairs each have different coding requirements.
- Documentation must clearly support wound depth, location, repair method, and total centimeters repaired.
- Modifier selection can significantly impact reimbursement.
- Accurate coding helps reduce denials and supports compliance with payer requirements.
- CPT and ICD-10-CM guidelines remain critical for coding accuracy in 2026.
Table of Contents
- What Is a Laceration?
- ICD-10-CM Coding for Lacerations
- CPT Coding for Laceration Repairs
- How to Measure Lacerations Correctly
- Modifier Usage for Laceration Repairs
- Billing Considerations for 2026
- Documentation Requirements
- Common Mistakes to Avoid
- CPC Exam Tips
- Additional Resources
- Frequently Asked Questions
What Is a Laceration?
A laceration is a tear or cut in the skin and underlying tissues caused by trauma. Depending on the severity, treatment may involve:
- Steri-strips
- Tissue adhesives
- Sutures
- Staples
- Layered closure
- Complex reconstruction
Consequently, coders must review the provider’s documentation carefully to determine the appropriate diagnosis and procedure codes.
ICD-10-CM Coding for Lacerations
The first step is assigning the correct ICD-10-CM diagnosis code.
Although many coders focus on the wound location, ICD-10-CM coding also requires documentation of:
- Anatomical site
- Laterality
- Foreign body status
- Encounter type
- Complications
Common ICD-10-CM Categories
| Body Region | ICD-10 Category |
|---|---|
| Head | S01.- |
| Neck | S11.- |
| Thorax | S21.- |
| Abdomen, lower back, pelvis | S31.- |
| Shoulder and upper arm | S41.- |
| Forearm | S51.- |
| Wrist and hand | S61.- |
| Hip and thigh | S71.- |
| Lower leg | S81.- |
| Ankle and foot | S91.- |
Furthermore, most laceration codes require a 7th character extension.
Encounter Extensions
| Extension | Meaning |
| A | Initial Encounter |
| D | Subsequent Encounter |
| S | Sequela |
Example
S61.011A – Laceration without foreign body of right thumb without damage to nail, initial encounter.
As a result, documentation must support:
- Right thumb
- No foreign body
- No nail involvement
- Initial treatment
Learn More
Related Article:
Medical Coding Steps for ICD-10-CM:
CPT Coding for Laceration Repairs
Once the diagnosis code is assigned, the next step is selecting the correct CPT repair code.
Importantly, CPT repair coding is based on:
- Complexity of repair
- Anatomical location
- Total wound length
Many coders mistakenly focus only on wound size. However, repair complexity is equally important.
Simple Repairs
Simple repairs involve:
- Epidermis
- Dermis
- Subcutaneous tissue only
- Single-layer closure
Common CPT Codes
| CPT Code | Description |
| 12001 | 2.5 cm or less |
| 12002 | 2.6 cm–7.5 cm |
| 12004 | 7.6 cm–12.5 cm |
| 12005 | 12.6 cm–20.0 cm |
Simple repair represents the most common type of laceration coding encountered in physician offices and urgent care settings.
Intermediate Repairs
Intermediate repairs require:
- Layered closure
- Deeper tissue involvement
- Extensive cleaning of heavily contaminated wounds
Common CPT Codes
| CPT Code | Description |
| 12031 | 2.5 cm or less |
| 12032 | 2.6 cm–7.5 cm |
| 12034 | 7.6 cm–12.5 cm |
| 12035 | 12.6 cm–20.0 cm |
Therefore, documentation must clearly state that layered closure was performed.
Complex Repairs
Complex repairs involve:
- Extensive undermining
- Retention sutures
- Scar revision
- Debridement beyond routine cleaning
- Significant reconstruction
Common CPT Codes
| CPT Code | Description |
| 13100 | Trunk repair up to 2.5 cm |
| 13101 | Each additional 5 cm |
| 13120 | Scalp, arms, or legs up to 2.5 cm |
| 13121 | Each additional 5 cm |
Consequently, providers must document the additional work that justifies reporting a complex repair.
Learn More
Medical Coding Steps for CPT:
https://codingclarified.com/medical-coding-steps-for-cpt/
How to Measure Lacerations Correctly
One of the most overlooked aspects of laceration coding is wound measurement.
According to CPT guidelines:
- Measure each repaired wound in centimeters.
- Add lengths of wounds in the same classification and anatomical grouping.
- Do not combine simple and intermediate repairs.
- Do not combine repairs from different anatomical groups.
Example
Simple Repairs:
- Forearm = 3 cm
- Forearm = 2 cm
Total length = 5 cm
Therefore, report 12002 rather than two separate repair codes.
Modifier Usage for Laceration Repairs
Modifiers may be necessary when additional procedures are performed.
Modifier 25
Used when a significant and separately identifiable E/M service is performed on the same day as the repair.
Example:
A patient receives a full injury evaluation and subsequently undergoes laceration repair.
Modifier 51
Used for multiple procedures when appropriate.
Modifier 59
Used to identify distinct procedural services that are not normally reported together.
Modifier 22
Used when documentation supports substantially greater work than typically required.
Learn More
Billing Considerations for 2026
As payer scrutiny continues to increase in 2026, documentation accuracy is more important than ever.
Additionally, coders should verify payer-specific policies regarding:
- Tissue adhesives
- Dermabond applications
- Wound debridement
- Foreign body removal
- Separate E/M reporting
Furthermore, some services that appear separately billable may be bundled under National Correct Coding Initiative (NCCI) edits.
Before billing, always verify current payer guidelines.
Medical Coding Aftercare and Follow-Up
ICD-10-CM distinguishes between active treatment and follow-up care.
Initial Encounter
Active treatment of the injury.
Example:
S61.011A
Subsequent Encounter
Routine healing phase.
Example:
S61.011D
Sequela
Long-term complications.
Example:
S61.011S
Related Article:
Medical Coding Aftercare and Follow-Up:
Documentation Requirements for Laceration Coding
Strong documentation supports both coding accuracy and reimbursement.
Providers should document:
Wound Location
Include exact anatomical site and laterality.
Wound Length
Document total centimeters repaired.
Wound Depth
Specify whether the repair is simple, intermediate, or complex.
Repair Method
Examples include:
- Sutures
- Staples
- Tissue adhesive
- Steri-strips
Foreign Body Status
Indicate whether a foreign body is present.
Complications
Document:
- Nerve injury
- Tendon injury
- Vascular injury
- Infection
Follow-Up Instructions
Include wound care instructions and planned follow-up visits.
Common Mistakes to Avoid
Even experienced coders make laceration coding errors.
Mistake #1: Coding Based Only on Wound Size
Always consider repair complexity.
Mistake #2: Missing the 7th Character
Most injury codes require an encounter extension.
Mistake #3: Combining Different Repair Types
Simple and intermediate repairs cannot be combined.
Mistake #4: Incorrect Modifier Usage
Improper modifier assignment frequently triggers denials.
Mistake #5: Insufficient Documentation
Lack of wound measurements often results in downcoding.
Mistake #6: Reporting Routine Cleaning Separately
Routine wound cleansing is included in the repair code.
CPC Student Tips
If you are preparing for the CPC exam, focus on the following:
Tip #1
Always identify the repair complexity before reviewing wound length.
Tip #2
Highlight CPT repair guidelines in your CPT manual.
Tip #3
Practice wound measurement scenarios frequently.
Tip #4
Memorize injury code 7th character requirements.
Tip #5
Review modifier usage regularly because modifier questions commonly appear on certification exams.
Tip #6
Watch for bundled services that may not be separately reportable.
Related Coding Clarified Articles
Expand your knowledge with these additional resources:
- ICD-10 Codes for Pain: Chronic, Acute, and Cancer-Related (2026)
- Anatomical Modifiers Guide: Finger, Toe, & Eyelid HCPCS Codes (2026 Update)
- Evaluation and Management (E/M) Guidelines for 2026: The Complete Guide
- Medical Coding Skin Substitutes
- Medical Coding Foreign Body
Additional Authoritative Resources
For official coding guidance, review:
Frequently Asked Questions About Laceration Coding
What CPT code is used for a simple laceration repair?
Simple laceration repairs are reported with CPT codes 12001–12018, depending on the anatomical location and total wound length.
How do I determine whether a repair is simple, intermediate, or complex?
The classification depends on the depth of repair and the amount of work performed. Layered closure generally indicates an intermediate repair, while extensive reconstruction may qualify as a complex repair.
Can multiple lacerations be added together?
Yes. However, only wounds within the same anatomical grouping and repair classification may be combined.
Is tissue adhesive coded separately?
In many situations, tissue adhesive closure is included within the appropriate repair code. Always verify payer-specific guidance.
When should Modifier 25 be reported?
Modifier 25 is appropriate when a significant and separately identifiable E/M service is performed on the same day as the laceration repair.
What is the most common reason for laceration claim denials?
Missing wound measurements, insufficient documentation, incorrect modifiers, and improper repair classification are among the most common causes of denials.
Do laceration diagnosis codes require a 7th character?
Yes. Most injury codes require a 7th character to indicate whether the encounter is initial, subsequent, or a sequela.
Are wound debridement services always separately billable?
No. Routine cleansing is included in the repair code. Separate reporting may be appropriate only when documentation supports a distinct and reportable debridement service.
Coding Clarified Final Thoughts
Medical coding for lacerations requires careful attention to diagnosis coding, repair complexity, wound measurements, modifier selection, and documentation. Moreover, as payer audits continue to increase in 2026, accurate coding has become even more important for protecting reimbursement and maintaining compliance. By following ICD-10-CM, CPT, NCCI, and payer-specific guidelines, coders can improve claim accuracy, reduce denials, and confidently report laceration repair services.