Evaluation and Management (E/M) Guidelines for 2026: The Complete Guide
By Janine Mothershed CPC, CPC-I
Key Takeaway: E/M Coding Changes for 2026
Effective January 1, 2026, Evaluation and Management (E/M) coding continues to emphasize Medical Decision Making (MDM) and total time selection while incorporating additional guidance for artificial intelligence (AI)-assisted documentation, expanded digital health services, and remote monitoring programs.
The most important updates include:
- Continued reliance on MDM or total time for code selection
- Greater recognition of physician cognitive work
- Additional guidance regarding AI-assisted documentation tools
- Expanded Remote Physiologic Monitoring (RPM) reporting
- Increased focus on documentation supporting medical necessity
- Clarification of provider responsibility when using AI-generated clinical insights
As a result, coders, auditors, physicians, and healthcare organizations must understand both traditional E/M coding principles and emerging healthcare technologies to remain compliant and maximize reimbursement.
Why the 2026 E/M Update Matters
Evaluation and Management services remain among the most frequently reported CPT® codes in healthcare. Consequently, even small documentation errors can result in claim denials, underpayments, overpayments, or audit risk.
While previous E/M reforms shifted coding away from history and examination scoring, the 2026 guidance further reinforces the importance of:
- Clinical judgment
- Medical necessity
- Data analysis
- Risk assessment
- Cognitive decision-making
- Technology-assisted healthcare delivery
Therefore, understanding these updates is essential for CPC students, practicing coders, auditors, physicians, nurse practitioners, physician assistants, and revenue cycle teams.
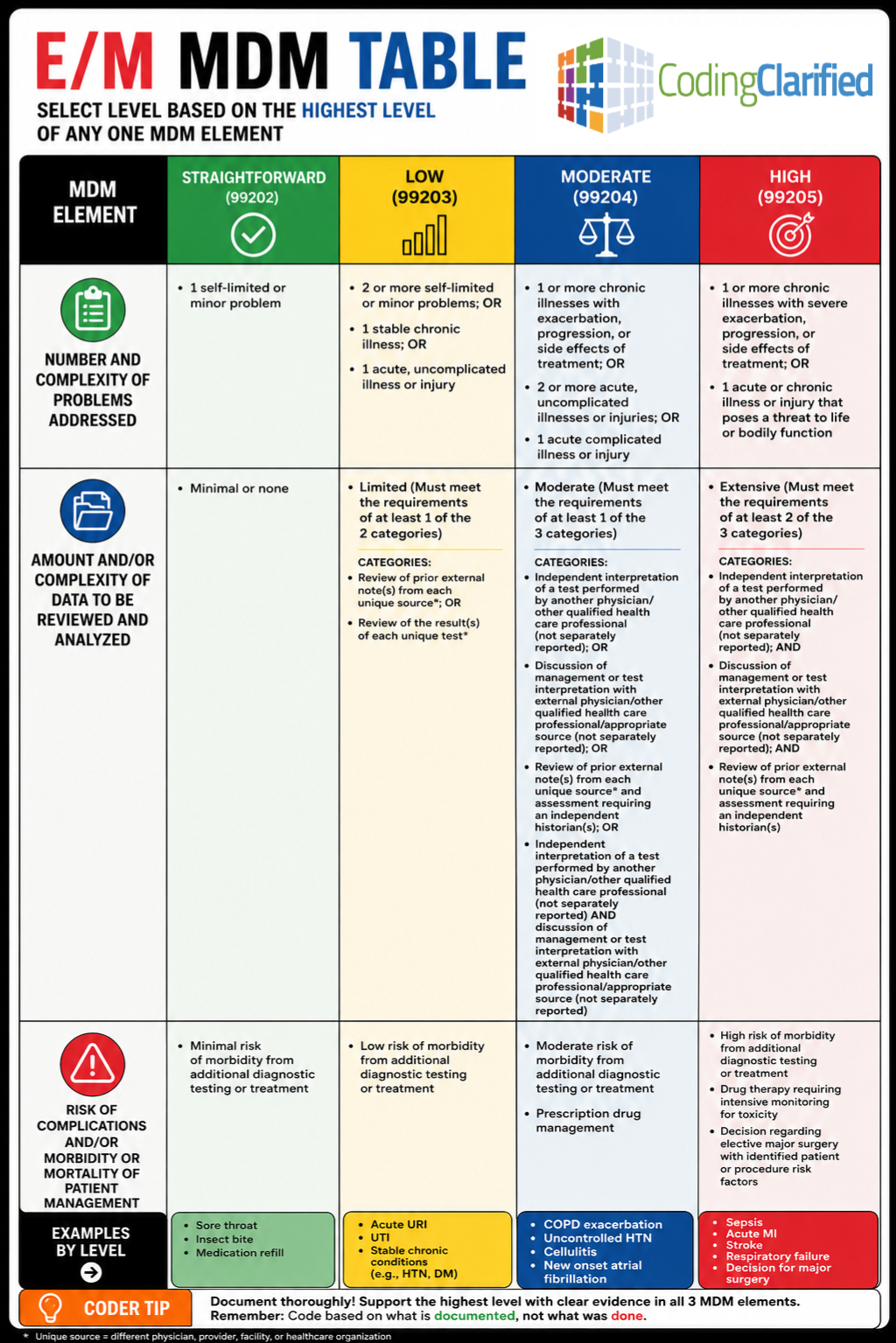
The 2026 E/M Medical Decision Making (MDM) Framework
Medical Decision Making remains the primary method of selecting most office and outpatient E/M codes.
The three MDM elements continue to include:
1. Number and Complexity of Problems Addressed
Providers must document the conditions evaluated and managed during the encounter.
Examples include:
- Stable chronic illnesses
- Acute uncomplicated illnesses
- Acute illnesses with systemic symptoms
- Chronic illnesses with exacerbation
- Conditions posing threats to life or bodily function
2. Amount and Complexity of Data Reviewed and Analyzed
The 2026 guidance continues to recognize:
- Laboratory studies
- Imaging studies
- External physician records
- Independent interpretations
- Discussions with external healthcare professionals
- Digital health and remote monitoring data
Additionally, AI-assisted data summaries may be reviewed; however, providers must still demonstrate independent clinical evaluation.
3. Risk of Complications and Morbidity
Risk assessment remains a major driver of E/M selection.
Examples include:
- Prescription drug management
- Minor surgery decisions
- Major surgery decisions
- Hospitalization decisions
- Escalation of treatment
- High-risk medication monitoring
AI-Assisted Documentation and E/M Coding in 2026
One of the biggest healthcare trends in 2026 is the rapid adoption of artificial intelligence tools.
Today, AI platforms may assist providers by:
- Summarizing patient encounters
- Organizing clinical data
- Suggesting diagnoses
- Highlighting documentation gaps
- Recommending E/M levels
However, coders must remember an important compliance principle:
AI cannot determine medical necessity.
Instead, providers must review, verify, and authenticate all AI-generated documentation.
Best Practice for Compliance
Documentation should clearly demonstrate:
- Provider review
- Independent interpretation
- Clinical reasoning
- Final treatment decisions
In other words, AI may support documentation, but physicians remain responsible for the medical record.
For additional guidance, review resources from the AMA and CMS regarding AI documentation practices.
Remote Physiologic Monitoring (RPM) Updates for 2026
Remote Physiologic Monitoring continues to grow as healthcare organizations expand virtual care services.
Unfortunately, many RPM resources discuss only device setup and monitoring. However, successful coding requires understanding the complete RPM code family.
CPT 99453
Initial setup and patient education on use of monitoring equipment
Used when:
- Equipment is supplied
- Patient receives education
- Monitoring program begins
CPT 99454
Device supply with collection, transmission, and programmed alerts
Used for:
- Physiologic data collection
- Daily recordings
- Device management
CPT 99457
Remote physiologic monitoring treatment management services, first 20 minutes
Requirements include:
- Interactive communication with the patient or caregiver
- Clinical staff, physician, or qualified healthcare professional involvement
- Minimum 20 minutes of treatment management time
CPT 99458
Each additional 20 minutes of RPM treatment management
Reported in conjunction with 99457 when additional time thresholds are met.
CPT 99091
Collection and interpretation of physiologic data digitally stored and transmitted by the patient
This code remains important for practices performing physician interpretation of physiologic data outside traditional RPM workflows.
Common RPM Documentation Requirements
Providers should document:
- Device usage
- Monitoring period
- Data transmission
- Interactive communication
- Clinical decision-making
- Total time spent
Because RPM services continue expanding in 2026, these codes are increasingly tested on certification exams and frequently audited by payers.
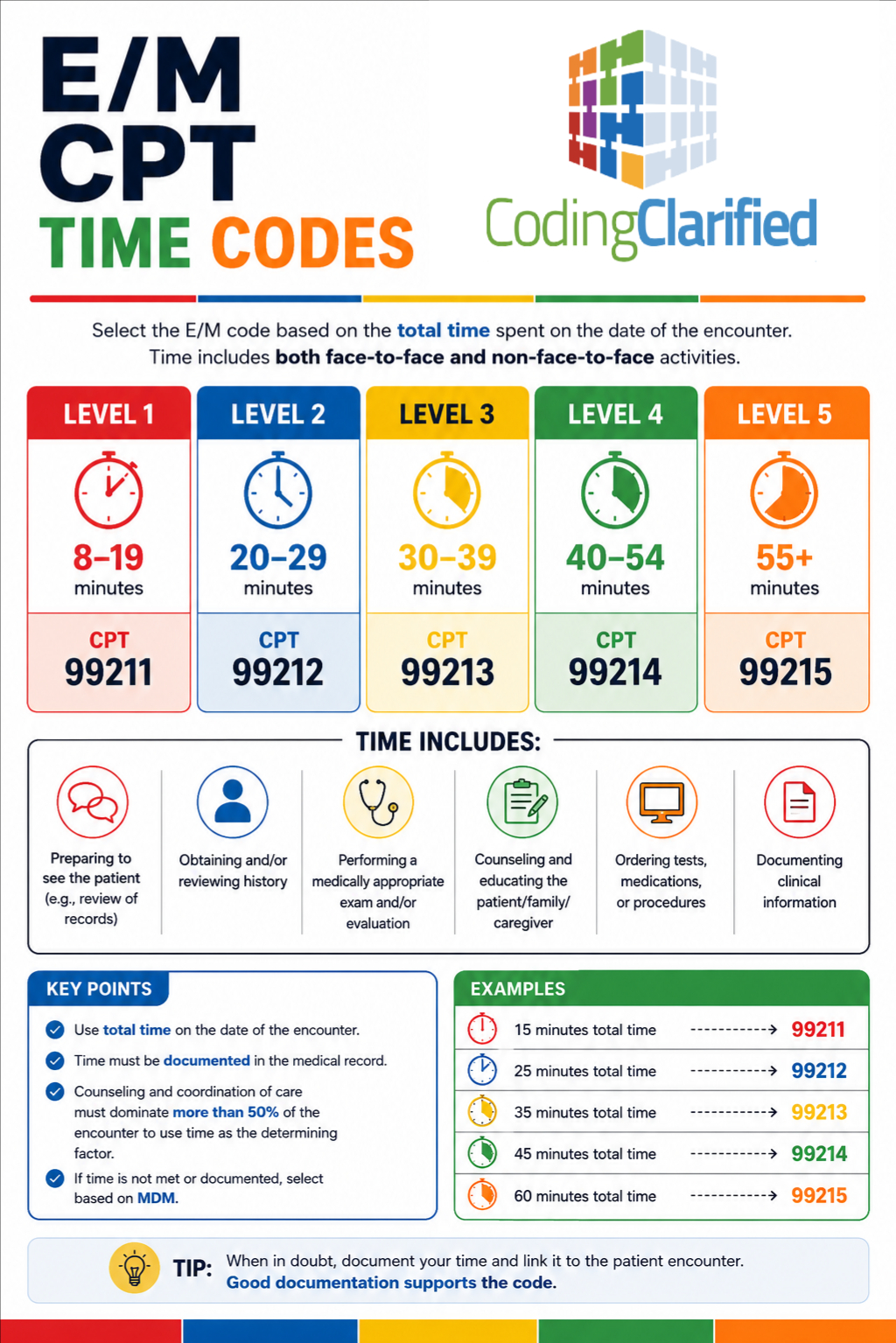
Total Time vs. Medical Decision Making in 2026
Providers may continue selecting many office E/M services based on either:
- Medical Decision Making (MDM)
- Total Time
However, only one method should be used to determine code selection.
When MDM Is Best
Choose MDM when:
- Multiple conditions are addressed
- Significant data review occurs
- Clinical complexity drives the visit
- Risk management is substantial
When Time Is Best
Choose time when:
- Counseling dominates the encounter
- Coordination of care is extensive
- Documentation clearly supports total time
- Complexity alone does not support a higher code
2026 Office Visit Time Thresholds
New Patients
| CPT Code | Total Time |
|---|---|
| 99202 | 15-29 minutes |
| 99203 | 30-44 minutes |
| 99204 | 45-59 minutes |
| 99205 | 60-74 minutes |
Established Patients
| CPT Code | Total Time |
| 99212 | 10-19 minutes |
| 99213 | 20-29 minutes |
| 99214 | 30-39 minutes |
| 99215 | 40-54 minutes |
Always verify the most current CPT® codebook for official reporting instructions.
Common E/M Coding Mistakes in 2026
Despite clearer guidance, several errors remain common.
Mistake #1: Over-Relying on AI
Coders should never assign codes solely because an AI platform suggested them.
Mistake #2: Confusing Data Review with Data Interpretation
Reviewing results and independently interpreting results are not always equivalent.
Mistake #3: Insufficient Time Documentation
Time-based coding requires documented total time.
Mistake #4: Ignoring Medical Necessity
Medical necessity remains the overarching criterion for payment.
Mistake #5: Missing Risk Documentation
The risk component often drives higher-level E/M services.
How to Stay Compliant with E/M Coding in 2026
Healthcare organizations should:
- Audit E/M claims regularly
- Educate providers on AI documentation
- Monitor payer policy updates
- Verify RPM requirements
- Review CPT® updates annually
- Focus on medical necessity
- Strengthen physician documentation training
Furthermore, coders should continually review AMA, CMS, and specialty-specific guidance to maintain compliance.
Authoritative Resources
For official guidance, review:
CMS Evaluation & Management Services
Related Coding Clarified Articles
Continue your E/M education with:
- Medical Coding Updates And Proposed Changes For Evaluation & Management (E/M) Coding In 2026
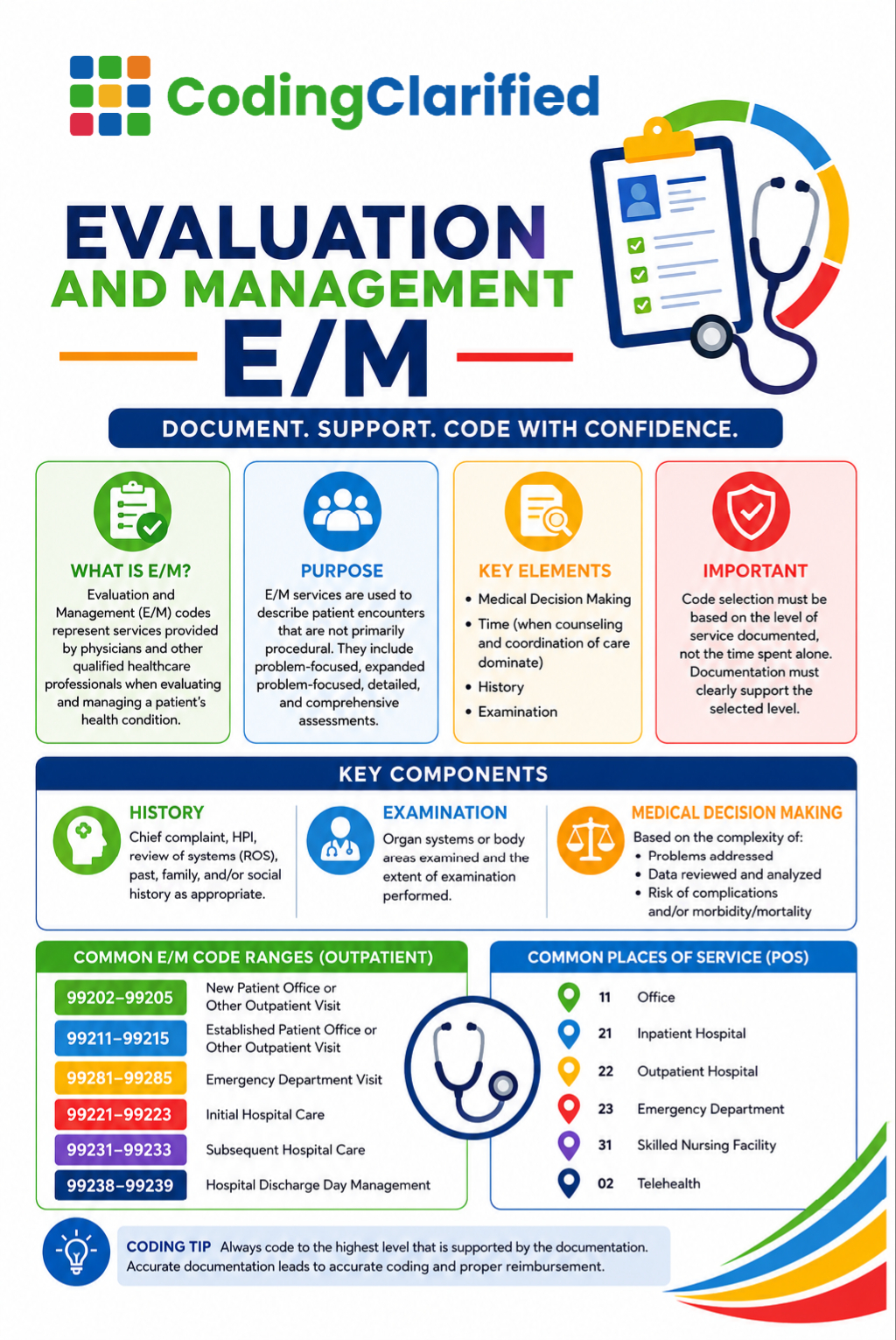
- What is Evaluation and Management (E/M) in Medical Coding
- Medical Coding E/M Prolonged Services
- How to Use the AAPC E/M Calculator
Browse all Coding Clarified Blog articles:
Frequently Asked Questions About E/M Coding in 2026
What changed in E/M coding from 2025 to 2026?
The biggest changes involve expanded guidance for AI-assisted documentation, increased recognition of physician cognitive work, clarification of digital health services, and additional focus on remote physiologic monitoring documentation and reporting.
What is the difference between MDM and time-based E/M coding?
MDM evaluates complexity based on problems addressed, data reviewed, and risk. Time-based coding relies on the total provider time spent on the date of the encounter. Providers may generally choose whichever method supports the highest appropriate code level.
What are the 2026 E/M time thresholds for office visits?
Established patient visits generally range from 10–19 minutes for 99212 through 40–54 minutes for 99215. New patient visits generally range from 15–29 minutes for 99202 through 60–74 minutes for 99205.
Can a provider use both MDM and time for the same visit?
A provider may document both. However, only one methodology should be used to select the final E/M code.
How does AI documentation affect E/M coding compliance?
AI tools may assist with documentation and data review, but providers remain responsible for reviewing, validating, and signing the final medical record. Medical necessity and physician judgment still determine code selection.
What is the most common E/M coding mistake in 2026?
One of the most common mistakes is selecting a code based solely on AI-generated recommendations without documentation supporting medical necessity and MDM requirements.
How do I choose between 99213, 99214, and 99215?
The decision depends on either the documented MDM level or total time. Generally, 99213 reflects low complexity, 99214 reflects moderate complexity, and 99215 reflects high complexity medical decision making.
Are RPM services separately billable from E/M visits?
In many circumstances, yes. However, providers must meet all CPT® requirements, document qualifying services, and ensure no payer-specific restrictions apply.
Cpdomg Clarified Final Thoughts
The 2026 E/M guidelines continue the healthcare industry’s movement toward value-based care, digital health integration, and accurate representation of physician cognitive work. Although AI tools and remote monitoring technologies are becoming increasingly common, successful coding still depends on thorough documentation, sound clinical judgment, and compliance with AMA and CMS requirements.
Coders who understand both traditional Medical Decision Making principles and emerging digital health services will be best positioned for long-term success in 2026 and beyond.