Medical Coding for Pain in 2026: Complete ICD-10-CM Guide to G89 and R52 Codes
By Janine Mothershed CPC, CPC-I
Key Takeaway: Pain Coding in 2026
Pain coding depends on three critical factors: documentation, encounter intent, and diagnosis sequencing. First, determine why the patient is being seen. Next, identify whether the encounter focuses on pain management or treatment of an underlying condition. Then, select the most specific ICD-10-CM code supported by provider documentation.
In most cases, coders will choose between:
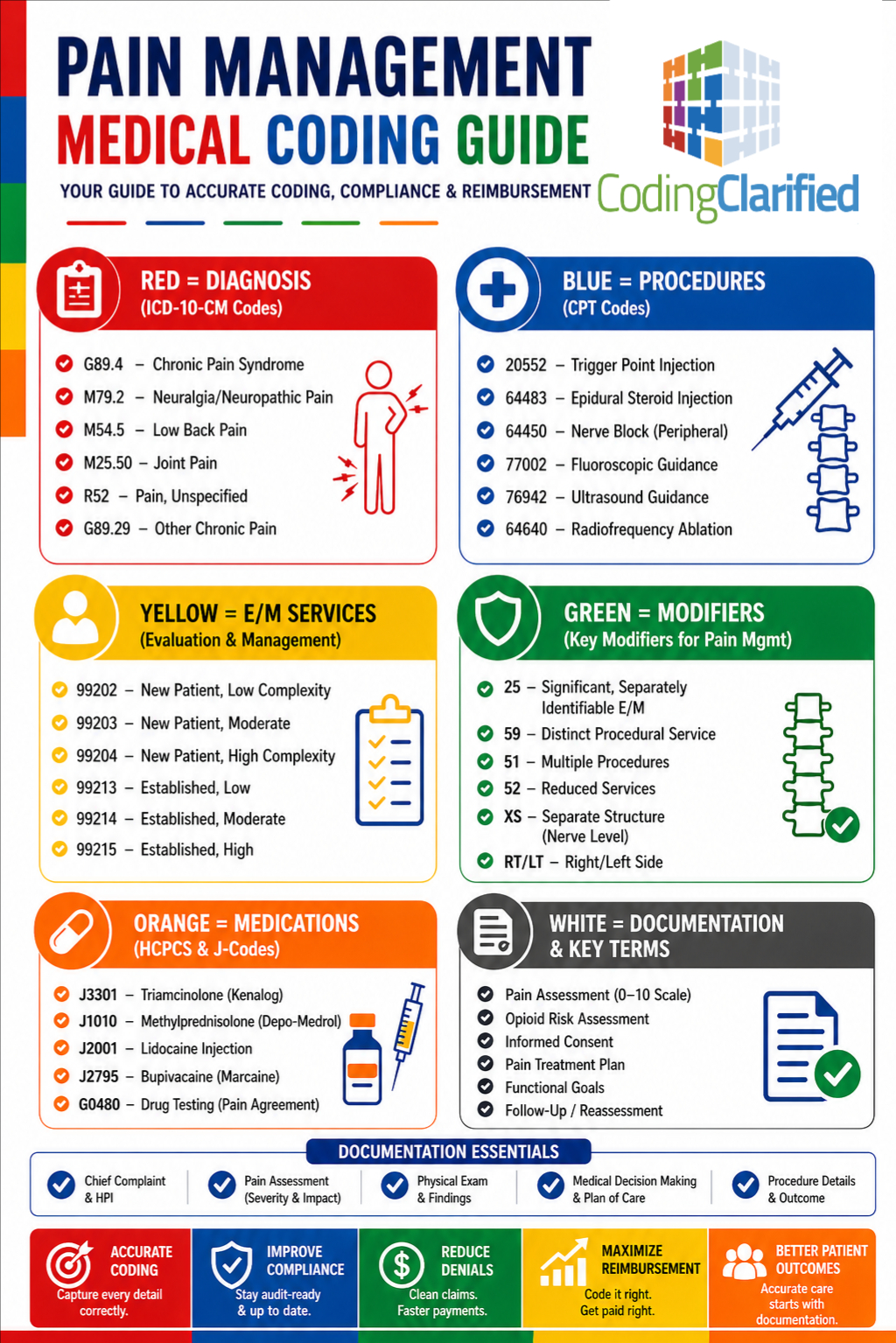
- Category G89 pain codes
- Site-specific pain codes
- R52 (Pain, unspecified)
Most importantly, coders should report a G89 code first only when pain management or pain control is the primary reason for the encounter.
As a result, understanding these guidelines can improve coding accuracy, reduce denials, and help CPC students answer pain-coding questions correctly on certification exams.
Why Pain Coding Matters in 2026
Pain remains one of the most common reasons patients seek medical care. Consequently, pain-related diagnoses appear across nearly every healthcare specialty, including orthopedics, oncology, neurology, rheumatology, pain management, and primary care.
Because pain affects such a large percentage of patient encounters, accurate diagnosis coding plays a significant role in reimbursement and compliance. Furthermore, pain coding errors frequently lead to claim denials, medical necessity issues, and audit findings.
Therefore, medical coders must understand not only the diagnosis codes themselves but also the sequencing rules that determine which diagnosis should appear first on the claim.
Additionally, CMS and commercial payers continue to emphasize documentation specificity. As a result, selecting the correct pain diagnosis has become even more important in 2026.
Understanding ICD-10-CM Category G89
Category G89 contains diagnosis codes that describe pain based on its type, duration, or cause. Unlike many symptom codes, G89 diagnoses provide additional information about the patient’s condition and often affect diagnosis sequencing.
However, coders should not automatically assign a G89 diagnosis whenever pain appears in the medical record. Instead, they should evaluate the purpose of the encounter and review the provider’s documentation carefully.
Generally, coders use G89 diagnoses when:
- The encounter focuses on pain control or pain management.
- The provider documents acute pain.
- The provider documents chronic pain.
- The provider diagnoses chronic pain syndrome.
- The provider links the pain to a malignancy.
- The provider documents postprocedural pain.
Consequently, understanding the distinctions within category G89 is essential for accurate coding.
Acute Pain Coding (G89.1-)
Acute pain typically develops suddenly and usually results from trauma, surgery, or a recent medical condition.
For example, common acute pain diagnoses include:
| ICD-10-CM Code | Description |
|---|---|
| G89.11 | Acute pain due to trauma |
| G89.18 | Other acute postprocedural pain |
Furthermore, coders should distinguish between routine postoperative discomfort and pain that requires separate treatment.
For instance, if a patient returns specifically for management of excessive postoperative pain, the provider may support assignment of G89.18.
However, coders should not automatically report expected postoperative pain separately.
Chronic Pain Coding (G89.2-)
Chronic pain often requires ongoing medical management and long-term treatment strategies. Nevertheless, coders should never assume pain is chronic based solely on duration.
Instead, the provider must specifically document chronic pain.
This distinction is important because many records contain phrases such as:
- Persistent pain
- Long-standing pain
- Pain for several months
Although these descriptions may suggest chronicity, they do not automatically support a chronic pain diagnosis.
Common chronic pain codes include:
| ICD-10-CM Code | Description |
|---|---|
| G89.21 | Chronic pain due to trauma |
| G89.29 | Other chronic pain |
Therefore, coders should always rely on provider documentation rather than personal interpretation.
Chronic Pain Syndrome vs. Chronic Pain
One of the most frequently tested CPC exam concepts involves the difference between chronic pain and chronic pain syndrome.
Although the terms sound similar, they represent different diagnoses.
G89.29 – Other Chronic Pain
Providers use this diagnosis when patients experience chronic pain that extends beyond the expected healing period.
G89.4 – Chronic Pain Syndrome
In contrast, chronic pain syndrome represents a more complex diagnosis involving physical, behavioral, emotional, and psychological factors.
Therefore, coders should assign G89.4 only when the provider specifically documents “chronic pain syndrome.”
This distinction frequently appears on CPC certification exams and in real-world coding audits.
Neoplasm-Related Pain (G89.3)
Cancer-related pain receives its own diagnosis code within category G89.
G89.3 – Neoplasm-Related Pain (Acute or Chronic)
Providers often document this diagnosis when cancer directly causes the patient’s pain.
Furthermore, coders must understand the sequencing rule associated with this diagnosis.
If the encounter focuses on pain control, coders should report G89.3 first and then report the underlying malignancy.
For example, a patient receiving treatment for metastatic cancer may present specifically for pain medication management. In that situation, G89.3 becomes the first-listed diagnosis.
Consequently, the diagnosis sequence accurately reflects the purpose of the encounter.
Postprocedural Pain Coding
Postprocedural pain coding often creates confusion for new coders.
Fortunately, the ICD-10-CM guidelines provide a straightforward approach.
First, determine whether the pain represents an expected outcome of the procedure.
If the pain falls within normal postoperative expectations, coders typically do not report it separately.
However, if the provider documents excessive pain, unusual pain, or pain requiring separate treatment, the provider may support assignment of an appropriate G89 diagnosis.
Therefore, documentation remains the key factor in determining whether separate coding is appropriate.
When Should Coders Use R52?
Although R52 appears simple, many coders overuse this diagnosis.
R52 – Pain, Unspecified
Coders should assign this code only when documentation lacks specificity.
For example, R52 may apply when:
- The provider documents generalized pain.
- The documentation does not identify a location.
- The provider does not identify a cause.
- No more specific pain diagnosis exists.
Conversely, coders should avoid R52 whenever documentation identifies a pain site, pain type, or underlying condition.
Therefore, coders should always select the most specific diagnosis available.
Site-Specific Pain Codes vs. G89 Codes
In many situations, site-specific pain diagnoses provide a more accurate coding option than R52.
Examples include:
| Pain Type | ICD-10-CM Category |
|---|---|
| Abdominal Pain | R10 |
| Chest Pain | R07 |
| Pelvic Pain | R10.2 |
| Low Back Pain | M54.50 |
| Joint Pain | M25.5 |
For example, if a patient presents with abdominal pain, coders should assign an R10 diagnosis rather than R52.
Likewise, coders should report chest pain using the appropriate R07 diagnosis.
However, when pain management itself becomes the focus of treatment, coders may need to assign both a G89 diagnosis and a site-specific pain diagnosis.
Pain Coding Sequencing Rules Every Coder Should Know
Sequencing remains one of the most important aspects of pain coding.
The following chart summarizes the most common scenarios:
| Scenario | First-Listed Diagnosis |
|---|---|
| Pain management encounter | G89 code |
| Underlying condition causes pain | Underlying condition |
| Cancer pain management | G89.3 |
| Site-specific pain encounter | Site-specific diagnosis |
| Generalized unspecified pain | R52 |
Because sequencing directly affects reimbursement and claim accuracy, coders should review these guidelines regularly.
Common Pain Coding Mistakes
Even experienced coders occasionally make pain coding errors.
Some of the most common mistakes include:
- Assuming pain is chronic without provider documentation
- Using R52 when a more specific diagnosis exists
- Sequencing G89 incorrectly
- Confusing G89.29 with G89.4
- Forgetting cancer-pain sequencing guidelines
Fortunately, careful documentation review can prevent most of these errors.
Related Coding Clarified Articles
To expand your coding knowledge, review these related resources:
- Medical Coding for Chronic Conditions
- Evaluation and Management (E/M) Guidelines for 2026: The Complete Guide
- Medical Coding MDM
- Essential Medical Coding Tools for Professionals
- Coding Clarified Blog
These topics frequently overlap with pain management documentation, medical necessity, and diagnosis sequencing.
Authoritative Resources
For official coding guidance, consult:
CMS Evaluation & Management Services
Additionally, coders should review the annual ICD-10-CM Official Guidelines for Coding and Reporting for the most current instructions.
Frequently Asked Questions About Pain Coding
What is the ICD-10 code for chronic pain?
G89.29 (Other chronic pain) is the most commonly assigned diagnosis when the provider documents chronic pain and no more specific chronic pain diagnosis applies.
What is the difference between G89.29 and G89.4?
G89.29 describes chronic pain, whereas G89.4 describes chronic pain syndrome, which includes additional behavioral and psychological components.
When should coders report G89 codes first?
Coders should report G89 diagnoses first when pain management or pain control serves as the primary purpose of the encounter.
When should coders use R52?
Coders should use R52 only when documentation identifies pain but does not identify a site, cause, or specific pain type.
Can coders assume chronic pain based on duration?
No. Providers must specifically document chronic pain before coders assign a chronic pain diagnosis.
How should coders report cancer-related pain?
Coders should assign G89.3. Furthermore, when pain control drives the encounter, they should sequence G89.3 before the malignancy diagnosis.
Can coders report a G89 code and a site-specific pain code together?
Yes. Depending on documentation and encounter circumstances, coders may report both diagnoses.
Is postoperative pain always coded separately?
No. Coders generally do not report expected postoperative pain separately. However, they may report unusual or excessive postoperative pain when documentation supports additional coding.
Coding Clarified Final Thoughts
Ultimately, accurate pain coding requires careful documentation review, proper sequencing, and a thorough understanding of ICD-10-CM guidelines. Moreover, coders should determine whether pain management drives the encounter or whether an underlying condition explains the patient’s symptoms.
Therefore, by mastering G89 diagnoses, site-specific pain diagnoses, and R52 guidelines, coders can improve coding accuracy, reduce denials, strengthen compliance, and perform more confidently on the CPC exam and in real-world coding environments.