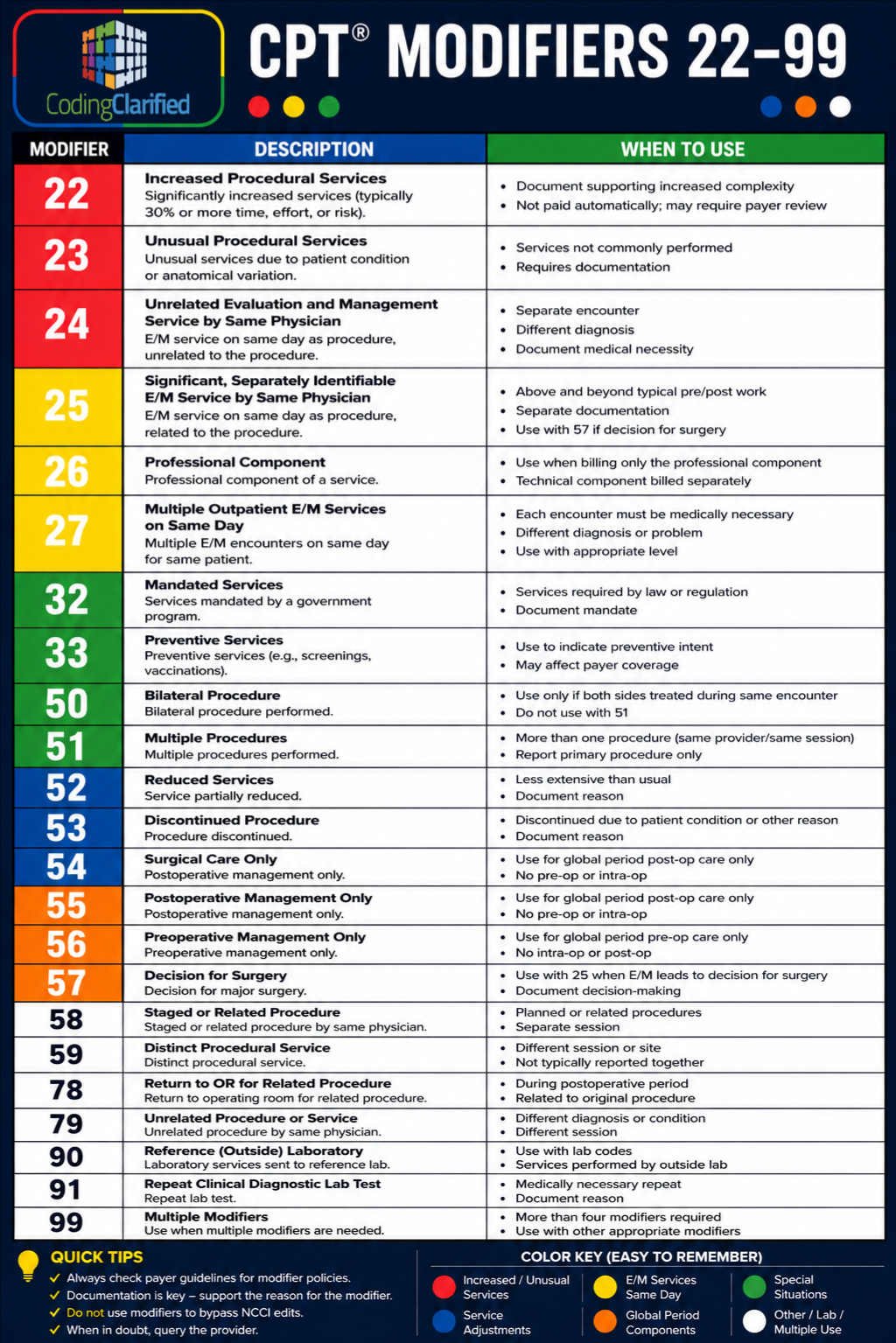
Understanding the Significance of CPT Modifiers in Medical Coding
Common CPT Modifiers
Anesthesia has its own modifiers that correspond to a patient’s health condition:
- P1– Normal, Healthy Patient
- P2– Patient with Mild Systemic Disease
- P3– Patient with Severe Systemic Disease
- P4– Patient with Severe Systemic Disease That is a Constant Threat to Life
- P5– Moribund patient who is not expected to survive without the operation
- P6– Declared brain-dead patient whose organs are being removed for donor
purposes
Review the proper use of each modifier.
Understand when each modifier should be applied.
- Procedure has both a professional and technical component
- Service is performed by more than 1 physician and/or in more than 1
location - Service has been increased or reduced
- Only part of a service was performed
- An adjunctive service was performed
- Service or procedure was provided more than once
- Unusual events occurred
- Service was provided during a global period but is NOT included as part of
the global reimbursement
CPT Modifier 22- Increased Procedural Services
Documentation must support the substantial additional work and the
reason for the additional work, which may include:
- Increased intensity
Time - Technical difficulty of procedure
- Severity of patient’s condition
- Physical and mental effort required
- Your documentation should provide our reviewers with a clinical picture of
the patient; the procedures/services performed and support the use of
modifier 22. Depending on the documentation, we may or may not allow
additional reimbursement. - Do not append modifier 22 to an E/M (Evaluation & Management) service;
only report it with procedure codes that have a global period of 0, 10, or 90
days.
CPT Modifier 23- Unusual Anesthesia
- Modifiers may only be submitted with anesthesia procedure codes (i.e.,
CPT codes 00100-01999). - Diagnostic bronchoscopy for mentally ill patients who become combative
CPT Modifier 24- Unrelated Evaluation and Management Service by the Same Physician or
Other Qualified
Modifier 24 is defined as an unrelated evaluation and management service
by the same physician or other qualified health care professional during a
post-operative period.
Medicare defines same physician as physicians in the same group practice
who are of the same specialty. In this instance they must bill and be paid as
though they were a single physician.
Modifier 24 is applied to two code sets:
- Evaluation and management (E/M) services (99202-99499).
- General ophthalmological services (92002-92014), which are eye
examination codes. - For unrelated critical care during the post-operative period refer to the FT
modifier. - Appropriate use
- Use Modifier 24 with the appropriate level of E/M service.
Use Modifier 24 on an E/M when:
An unrelated E/M service is performed beginning the day after the
procedure, by the same physician, during the 10 or 90-day post-operative
period.
Documentation indicates the service was exclusively for treatment of the
underlying condition and not for post-operative care.
The same physician is managing immunosuppressant therapy during the
post-operative period of a transplant.
The same physician is managing chemotherapy during the post-operative
period of a procedure.
The same diagnosis as the original procedure could be used for the new
E/M if the problem occurs at a different anatomical site.
Inappropriate use
Do not use Modifier 24 when:
- The E/M is for a surgical complication or infection, removal of sutures, or other wound treatment. These treatments are part of the surgery package.
- The surgeon admits a patient to a skilled nursing facility for a condition related to the surgery.
- The medical record documentation clearly indicates the E/M is related to the surgery. Outside of the post-op period of a procedure.
- Services are rendered on the same day as the procedure.
- Reporting exams performed for routine postoperative care.
- Reporting surgical procedures, labs, x-rays, or supply codes.
- Health Care Professional During a Postoperative Period
CPT Modifier 25- Significant, Separately Identifiable Evaluation and Management Service by the Same Physician or Other Qualified Health Care Professional on the Same Day of the Procedure or Other Service
- Often questions are posed regarding whether to bill an E/M visit on the same
day as a procedure and/or other services with modifier 25. - Are there signs, symptoms, and/or conditions the physician or the other
qualified health care professional must address before deciding to perform
a procedure or service? - If Yes, based on the documentation, an E/M service might be medically
necessary with modifier 25 - Were the physician’s or other qualified health care professional’s evaluation
and management of the problem significant and beyond the normal
preoperative and postoperative work? - If Yes, an E/M may be billed with modifier 25
- If No, it is not appropriate to bill with modifier 25
CPT Modifier 26- Professional Component
- Modifier 26 is defined as the professional component (PC).
- The PC is outlined as a physician’s service, which may include technician
supervision, interpretation of results and a written report. - Use modifier 26 when a physician interprets but does not perform the test.
- Most radiology codes, including ultrasounds, x-rays, CT scans, magnetic
resonance angiography, and magnetic resonance imaging, may be billed with
modifier 26 or TC, or with no modifier at all, indicating that the provider
performed both the professional and technical services.
indicates that a physician has interpreted the results of a test when they did
not personally perform it. Modifier 26 is the professional component (PC) of
a procedure. The PC is outlined as a physician’s service, which may include
technician supervision, interpretation of results, and a written report. - Is appended to billed codes to indicate that only the professional component
of a service/procedure has been provided. For example, if a facility provides
the technical component of a service/procedure, while an individual
physician performs the professional component, they should report the code
with modifier -26. - Modifier 26 should always be added before any other modifier
- This modifier must be reported in the first modifier field.
Appropriate use of Modifier 26
- When billing only the professional component portion of a test
- To report the physician’s interpretation of a test
- Procedures that have a “1” in the Professional Component (PC)TC field on
- the Medicare Physician Fee Schedule Database (MPFSDB)
Procedures falling into the following types of service:
1 – Medical Care/Injections
2 – Surgery
4 – Radiology
5 – Lab
6 – Radiation Therapy
8 – Assistant Surgeon
Inappropriate use of Modifier 26:
- Evaluation and management (E/M) or anesthesia codes
Procedure or service descriptors that indicate professional component only - Global test only codes, example: CPT 93000.
- Professional component only codes. PC/TC indicator 2 of MPFSDB denotes a
professional component only code that identifies stand-alone codes. - An example of a professional component only code is 93010,
Electrocardiogram; interpretation and report. Modifier 26 cannot be used
with this code. - Re-read results of an interpretation provided by another physician.
CPT Modifier 27-Multiple Outpatient Hospital E/M Encounters on the Same Date
- Append modifier 27 when reporting multiple outpatient hospital evaluation
and management (E/M) services on the same date. - Modifier 27 was created exclusively for hospital outpatient departments
(ex. hospital emergency department, clinic, and critical care). - Note: Physician practices may not use this modifier. This modifier should
only be reported on the UB-04 Part A claim form or electronic equivalent. - Hospitals may append modifier 27 to the second and subsequent E/M code
to indicate that the E/M service is a “separate and distinct E/M encounter”
from the service previously provided that same day in the same or different
hospital setting. - Hospitals may append modifier 27 to the range of E/M service codes listed
below.- 92002-92014 (Ophthalmological E/M services)
- 99281-99285 (Hospital type A emergency department visits)
- 99291-99292 (Critical care)
- G0175 (Interdisciplinary team conference)
- G0380-G0384 (Hospital type B emergency department visits)
- G0402 (Initial preventive physical examination)
- G0463 (Hospital outpatient clinic visit for assessment and management)
- Report condition code G0 (zero) with modifier 27 when multiple medical
visits occur on the same day in the same revenue centers.
CPT Modifier 32 – Mandated Services
Is used only whenever a service has to be extended to a third party entity
or in the case of Worker’s Compensation or some other such official entity.
However, modifier 32 may never be used when the patient wishes to seek a
second opinion from a different doctor.
CPT Modifier 33 – Preventative Services
Used to identify medical care whose primary purpose is delivery of an
evidence-based service, based on recommendations from the US
Preventive Services Task Force.
CPT Modifier 47 – Anesthesia by Surgeon
This modifier may be submitted when the operating surgeon performs the
anesthesia service (does not include local anesthesia). Add CPT modifier 47
to the basic service for regional or general anesthesia provided by the
surgeon.
CPT Modifier 50 – Bilateral Procedures
- Modifier 50 is used to report bilateral procedures that are performed
during the same operative session by the same physician. - These procedures can be performed on both sides of the body, such as the
spine, skull, or nose. - Modifier 50 is used as a payment modifier, rather than an informational
modifier. It can affect payment depending on the procedure code and the
BILAT SURG indicator. - Modifier 50 can be used when two procedures are reported using the same
CPT code and are performed on both sides of a single, symmetrical
structure or organ. For example, modifier 50 can be used when two
procedures on the spine or skull are performed using the same CPT code. - Modifier 50 is not reported when a procedure is identified as bilateral or
unilateral
CPT Modifier 51 – Multiple Procedures (some multiple surgical procedures must be reported WITHOUT modifier 51 identified as add-on codes – appendix I)
• Modifier 51 is used to indicate that the same provider performed multiple
procedures on the same day during the same session. This includes
procedures other than E/M services, such as physical medicine and
rehabilitation services or supplies.
• Modifier 51 is a Medicare contractor assigned modifier. Medicare does not
recommend reporting modifier 51 on your claim submission.
• You should list the most resource-intense (highest paying) procedure first,
and append modifier 51 to the second and subsequent procedures
• Multiple surgeries performed on the same day, during the same surgical
session.
• Diagnostic Imaging Services subject to the Multiple Procedure Payment
Reduction that are provided on the same day, during the same session by
the same provider.
• Note: Medicare doesn’t recommend reporting Modifier 51 on your claim;
our processing system will append the modifier to the correct procedure
code as appropriate.
Appropriate Usage of CPT Code Modifier 51
- The same physician performs more than one surgical service at the same
session (Indicator 2) - The technical component of multiple diagnostic procedures, Multiple
Procedure Payment Reduction (MPPR) rule applies (Indicator 4). - The multiple surgical procedures are done on same day but billed on two
separate claims. - The surgical procedure code is the lower physician fee schedule amount.
- The diagnostic imaging procedure with the lower technical component fee
schedule amount.
Inappropriate Use of CPT Code Modifier 51
- Do not append to add-on codes (See Appendix D of the CPT manual)
- Do not report on all lines of service
- Do not append when two or more physicians each perform distinctly,
different, unrelated surgeries on the same day to the same patient.
Additional Information - Medicare pays for multiple surgeries by ranking from the highest physician
fee schedule amount to the lowest physician fee schedule amount. - 100% of the highest physician fee schedule amount
- 50% of the physician fee schedule amount for each of the other codes
- Medicare will forward the claim information showing Modifier 51 to the
secondary insurance. - Multiple surgery pricing also applies to assistant at surgery services.
- Multiple surgery pricing applies to bilateral services (modifier 50)
performed on the same day with other procedures.
CPT Modifier 52 – Reduced Services
Under certain circumstances a service or procedure is partially reduced or
eliminated at the provider’s discretion.
- Modifier 52 is used to indicate a partial reduction or discontinuation of
radiology procedures or services that do not require anesthesia. This can be
used when a physician elects to partially reduce or discontinue a procedure
for reasons other than the patient’s well being being threatened. - Modifier 52 is outlined for use with surgical or diagnostic CPT codes. It can
be used when a procedure has an existing CPT code, but not all of the
components of the code were performed. For example, if the patient only
receives 30 minutes of PT instead of the 45 minutes that was scheduled. - Procedure codes submitted with modifier 52 will be reimbursed at a
reduced rate. Health plans reimburses procedure(s) appended with
modifier 52 at 50% of the allowable amount
Appropriate usage of CPT Code 52 – Reduced Services
- The service performed was significantly less than usually required.
- To indicate partial reduction of services for which anesthesia is not
planned. - Append modifier to the reduced procedure’s CPT code.
- Ambulatory surgical centers (ASC) use modifier 52 to indicate the
discontinuance of a procedure not requiring anesthesia. - Contractors apply a 50 percent payment reduction for discontinued
radiology and other procedures not requiring anesthesia. - ASC services billed with modifier -52 modifier are not subject to the
multiple procedure reduction.
Inappropriate Use of CPT Code 52 Reduced Services
- To report the termination of a procedure.
- Do not use on time-based codes.
- When used on evaluation and management services.
Supporting documentation - Additional information to support the modifier can be written in the
narrative of claim - If data cannot be written in the narrative, documentation must be
submitted. - Supporting documentation should:
- State when the procedure was started.
- Explain why the procedure was discontinued.
- Notate the percentage of the procedure that was performed.
CPT Modifier 53- Discontinued Procedure
Under certain circumstances, the provider may elect to terminate a surgical
or diagnostic procedure due to circumstances that may threaten the wellbeing of the patient.
Appropriate Use of CPT Modifier 53
- A discontinued procedure after induction of anesthesia.
- Append modifier to the discontinued procedure’s CPT code.
Inappropriate usage - Reporting on an evaluation and management (E/M) procedure code
- Discontinued surgeries prior to the administration of anesthesia
- Do not use on time-based procedure codes (i.e., anesthesia, critical care
and psychotherapy) - Used for services in an ambulatory surgery center or a hospital outpatient
department
Supporting documentation - Additional information to support the modifier can be written in the
narrative of claim - If data cannot be written in the narrative, documentation must be
submitted. - State when the procedure was started.
- Explain why the procedure was discontinued.
- Notate the percentage of the procedure that was performed.
CPT Modifier 54 – Surgical Care Only & 55- Postoperative Management Only
Global package
- Physicians who perform the surgery and furnish all the usual pre- and postoperative work should bill for global surgical care by using the proper CPT surgical code(s). In this situation physicians should not bill separately for visits or other services that are included in the global package. No modifier is necessary.
- When different physicians in a group practice participate in the care of the patient and all the physicians reassign benefits to the group, the group bills for the entire global package. The physician who performs the surgery is shown as the performing physician. No modifier is necessary
Co-management
- Occasionally a physician must transfer the care of the patient during the global care period. In these instances, the use of a modifier will be necessary to distinguish who is providing care for the patient. Novitas expects these instances to be rare.
Reasons for splitting care
- The operating surgeon is unavailable after surgery and the patient’s
postoperative care has to be managed by another physician. - The patient is unable to travel the distance to the surgeon’s office for
postoperative care visits. - The care is provided in a health professional shortage area (HPSA) and the
patient is unable to travel to the surgeon’s office. - The surgeon practices in a site remote from where the patient recuperates, e.g., the surgery is performed in a remote area and the surgeon does not return to the area frequently enough to provide the preoperative or postoperative care.
- The patient voluntarily wishes to be followed postoperatively by another physician.
- The surgery is performed by an itinerant surgeon in a remote area of the country.
Transfer of postoperative care is not covered if
- The operating surgeon is available, and he/she can manage other patients
postoperatively unless the patient voluntarily wishes to be followed
postoperatively by another provider. - The surgeon does follow the patient postoperatively but splits the fee with
another provider. - Two or more physicians co-manage patients indiscriminately as a matter o
policy and not on a case-by-case basis. - A physician demands to manage the postoperative care and indicates that
he/she will withhold making referrals to surgeons who would not agree to
split global surgery payments. - A surgeon opts to transfer postoperative care.
- The transfer is not made in writing.
- The transfer of care is used as an incentive for obtaining referrals from providers to receive postoperative care reimbursement.
- The patient has not consented to the transfer of care even after being apprised of the medical and/or logistic advisability or the risks and benefits of transfer care.
Surgical care for CPT Modifier 54
- Specific billing guidelines must be followed when the surgical procedure
and post-operative care is split between different physicians. Modifiers 54
and 55 are used to indicate two different physicians are rendering the
surgical care and post-operative management services. Where physicians
agree on transfer of care during a 10-day or 90-day global period, the
following modifiers are used: - 54 for surgical care only, or
- 55 for postoperative management only
- Physician rendering:
- One-day preoperative care
- Intraoperative services
- Any in-hospital visits
- Bill services with:
- Date of the surgery
- Procedure code for the surgery
- 54 modifier to indicate that the bill is reflective only of the surgical care
- If the physician who performed the surgery relinquishes care any time after
the surgery, the date of the transfer of care must be indicated in item 19 or
the equivalent for electronic submission.
Postoperative/Out of hospital care for CPT Modifier 54
Bill services with:
- Date of the surgery
- Procedure code for the surgery
- 55 modifier
In the case where the surgeon also cares for the patient for some period following discharge, the surgeon should bill the surgery with a 55 modifier and indicate the portion of the post-operative care provided in addition to the surgery with a 54 modifier (to indicate the intra-operative service). In those cases where the postoperative care is “split” between physicians, the billing for the postoperative care should be reported as follows:
- Report the date of service using the date of the surgical procedure.
- Report the procedure code for the surgical procedure, followed by modifier 55.
- Report the date the post-operative care began and ended along with the number of post-operative care days in the narrative field of electronic claims, or item 19 on the CMS 1500 claim form or the electronic equivalent.
- When there is a transfer of postoperative care, Medicare regulations require a written transfer of care agreement between the operating surgeon and the physician assuming care. Both the surgeon and the physician(s) providing the post-operative care must keep a copy of the written transfer agreement in the beneficiary’s medical records.
- Where a transfer of postoperative care occurs, the receiving physician cannot bill for any part of the global services until he/she has provided at least one service. Once the physician has seen the patient, that physician may bill for the period beginning with the date on which he/she assumes care of the patient using the surgery date as the billed date of service.
Both bills for surgical care only and postoperative care only, must contain:
- Same date of service
- Same surgical procedure code
- Appropriate modifier
- Note: Providers must report the date when post-operative care is assumed
from another provider including the date post-operative care began and
ended along with the number of post-operative care days provided in the
narrative field on electronic claims, or item 19 on the CMS 1500 claim form.
This will facilitate processing of the claim and reduce unnecessary
rejections.
CPT Modifier 56 – Preoperative Management Only
Is used by a physician or other qualified healthcare professional who
performs preoperative care but does not provide the intraoperative
(Surgical) or postoperative services.
CPT Modifier 57 – Decision for Surgery
CPT Modifier 57 is used to:
Indicate that documentation is available in the patient’s records to support the E/M service. Modifier 57 is used to indicate an Evaluation and Management (E/M) service resulted in the initial decision to perform surgery either the day before a major surgery (90 day global) or the day of a major surgery.
Appropriate Use of CPT Modifier 57
Append, only to the E/M procedure code, where the decision to perform surgery
is made the day of or day before a major surgery during an E/M service.
Inappropriate Use of CPT Modifier 57
- Appending to a surgical procedure code.
- Appending to an E/M procedure code performed the same day as a minor
surgery. - When the decision to perform a minor procedure is done immediately before the service, it is considered a routine preoperative service and not billable in addition to the procedure.
- Do not report on the day of surgery for a preplanned or prescheduled surgery.
- Do not report on the day of surgery if the surgical procedure indicates performance in multiple sessions or stages.
Global period includes:
- Day before surgery
- Day of the surgery; and
- Number of days following the surgery
- Note: A major surgery has a 90 day post-operative period and a minor surgery has either a zero or a 10 day post-operative period.
- Preoperative period is the day before the surgery or the day of surgery E/M service resulting in initial decision to perform major surgery is furnished during post-operative period of another unrelated procedure, then the E/M service must be billed with both the 24 and 57 modifiers.
CPT Modifier 58- Staged or Related Procedure or Service by the Same Physician During the
Postoperative Period
Planned, either at the time of the first procedure or prospectively
• More extensive than the first procedure
• A new postoperative period begins when the staged procedure is billed.
Appropriate use
Report when a procedure or service during the postoperative period was:
• Planned prospectively or at the time of the original procedure.
• More extensive than original procedure.
• For therapy following a diagnostic surgical procedure.
• When performing a second or related procedure during the postoperative
period.
Inappropriate use
• Staged procedures do not apply to claims for assistant at surgery.
• Appending the modifier to ambulatory surgical center (ASC) facility fee
claims.
• Doesn’t apply to procedures with XXX global period.
• Unrelated procedures during the postoperative period.
• Reporting the treatment of a complication from original surgery that
requires a return to operating room or service not separately payable that
does not require a return to the operating room.
59- Distinct Procedural Service
This means that a procedure or service was distinct or independent from other
services performed on the same day. Modifier 59 is used for procedures or
services that are not normally reported together, but are appropriate and
separately billable given the circumstances.
Modifier 59 can be used to distinguish:
- A different session or patient encounter
- A different procedure or surgery
- A different anatomical site
- A separate injury
- When an intravenous (IV) protocol calls for two separate IV sites
CPT Modifier 62 -Two Surgeons
- Indicates when two surgeons work together as primary surgeons on a single reportable procedure. Each surgeon must add modifier 62 to the same procedure code. Modifier 62 indicates that two or more surgeons were required for the same procedure on the same patient, during the same operative session, and on the same date of service.
- For example, modifier 62 would be used when one surgeon makes an incision and exposes the area requiring surgery, and another surgeon performs the surgery. Modifier 62 can also be used for co-surgery, where two surgeons perform parts of a procedure simultaneously, such as a heart transplant.
- Modifier 62 must be on both claims. If it is not, one physician will be paid at 100% and the other physician’s claim will be denied.
- Medical records must demonstrate why a co-surgeon or assistant was needed during the surgery.
CPT Modifier 63- Procedure Performed on Infants less than 4 kg.
Represents procedures performed on neonates and infants up to a present
body weight of 4 kilograms.
CPT Modifier 66- Surgical Team
- If a team of surgeons (more than two surgeons of different specialties) is
required to perform a specific procedure, each surgeon bills for the
procedure with a modifier 66. - Documentation is required to support claims submitted with this modifier.
- Note: The documentation should include each surgeon’s description of
their role in the performance of the surgery.
Correct Use of CPT Modifier 66
- Includes other highly skilled and specially trained personnel
- Includes different types of complex equipment
- Usually confined to organ transplant teams
- Reimbursed “by report”
- Medicare Physician Fee Schedule (MPFS) Indicator List:
- 0 – Team surgeons not permitted for this procedure.
- 1 – Team surgeons could be paid; supporting documentation required to
establish medical necessity of a team; pay by report. - 2 – Team surgeons permitted; pay by report.
Every surgeon must append modifier 66 to the CPT code.
Incorrect Use CPT Modifier 66
CPT Modifier 66 should not be used for two or less surgeon
CPT Modifier 73- Discontinued Outpatient Hospital/Ambulatory Surgery Center (ASC)
Procedure Prior to the Administration of Anesthesia
Physicians should not use this modifier.
This is only appropriate for use by the ASC.
Appropriate Usage of CPT Modifier 73
Due to extenuating circumstances or threaten patient well-being:
- Prior to procedure started/patient’s surgical preparation (including
sedation or taken to procedure room) - Prior to administration of anesthesia (local, regional block or general)
Inappropriate Usage of CPT Modifier 73
- Physician cancelled the surgical or diagnostic procedure prior to administration of anesthesia and/or surgical preparation of the patient
- Elective cancellation of a procedure
- Surgeon cancels or postpones because patient complained of a cold or flu upon intake
CPT Modifier 74- Discontinued Outpatient Hospital/Ambulatory Surgery Center (ASC) Procedure After the Administration of Anesthesia
- The patient must be prepared for the procedure and taken to the room
where the procedure is to be performed - This modifier is not for physician use. It is only appropriate for the ASC.
- For physician reporting of discontinued procedures, refer to modifier 53.
Appropriate usage of CPT Modifier 74
- may terminate surgical/diagnostic procedure after procedure starts
(incision made, intubation started, scope inserted), and after
administration of anesthesia (local, regional block or general).
Inappropriate usage of CPT Modifier 74
- Elective cancellation or postponement of a procedure based on the
physician or patient’s choice - Termination of the procedure prior to the beginning of the procedure or the
administration of anesthesia
CPT Modifier 76 -Repeat Procedure by Same Physician or Other Qualified Health Care Professional
- Modifier 76 defines a repeat procedure or service, on the same day, by the
same physician or other qualified healthcare professional (QHP). - Use modifier 76 to indicate a procedure or service was repeated subsequent to the original procedure or service.
- Claim submission instructions if performing repeat procedures on the same day by the same physician or other QHP:
- Use modifier 76 on a separate claim line with the number of repeated services.
- Do not report modifier 76 on multiple claim lines, to avoid duplicate claim line denials.
- Bill all services performed on one day on the same claim, to avoid duplicate claim denials.
- Documentation must support the use of the modifier.
CPT Modifier 77- Repeat Procedure by Another Physician or Other Qualified Health Care Professional
Modifier 77 is defined as a repeat procedure or service by another physician or other qualified healthcare professional. Used to indicate a procedure or service was repeated by another physical or other qualified healthcare professional. Indicate that a basic procedure or service had to be repeated.
Appropriate uses of CPT Modifier 77
- Add modifier 77 to the professional component of an x-ray or electrocardiogram (EKG) procedure when the patient has two or more tests and/or more than one physician provides the interpretation and report.
- We will reimburse a second interpretation of the same EKG or x-ray only under unusual circumstances, such as:
- A questionable finding for which the physician performing the initial interpretation believes another physician’s expertise is needed, or
- A change in diagnosis resulting from a second interpretation
- Note: Absent these circumstances, we will reimburse only the interpretation and report that directly contributed to the diagnosis and treatment of the individual patient.
Inappropriate uses of CPT Modifier 77
- Billing for multiple services which are considered bundled.
- Appending Modifier 77 to an evaluation and management code.
Claim submission instructions
If performing repeat procedures on the same day:
- Report each procedure on separate lines.
- List the procedure code once by itself and then again with modifier 77.
- Do not use the units’ field to indicate the procedure was performed more than once on the same day.
- Add modifier 77 when billing for multiple services on a single day and the service cannot be quantity billed.
- Report the unusual circumstance to support the use of the modifier in the narrative description
- If data cannot be written in the narrative, documentation must be submitted.
- Failure to report modifier 77 and the unusual circumstances in the narrative portion of the claim or the EDI equivalent will result in a claim rejection.
CPT Modifier 78- Unplanned Return to the Operating Room by Same Physician or Other Qualified Health Care Professional Following Initial Procedure for a Related Procedure During the Postoperative Period
Appropriate usage of CPT Modifier 78
- To identify a related procedure (that has 10 or 90 global surgery period) requiring a return trip to the operating room within the postoperative period of a major or minor surgery.
- To treat the patient for complications resulting from the original surgery
- When the procedure code used to describe a service for a treatment of complications is the same as the procedure code used in the original procedure.
Inappropriate usage
On any procedure code that does not have global period of 0010 or 0090.
• When surgery is unrelated to the original procedure.
• On procedures performed in any place other than the operating room.
• On ambulatory surgical center (ASC) facility services.
Facts About CPT Modifier 78
- An operating room (OR) is defined as a place of service specifically equipped and staffed for the sole purpose of performing procedures. The term includes a cardiac catheterization suite, a laser suite, and an endoscopy suite. It does not include a patient’s room, a minor treatment room, a recovery room, or an intensive care unit (unless the patient’s condition was so critical there would be insufficient time for transportation to the OR).
- Modifier 78 allows for the intraoperative percentage only of major or minor procedures (010 or 090 global periods).
- A new postoperative period does not begin when using modifier 78.
- Medicare allows codes with global surgery indicators of XXX and ZZZ in the Medicare Physician Fee Schedule (MPFS) database separately without modifier 78.
CPT Modifier 79- Unrelated Procedure or Service by the Same Physician or Other Qualified Health Care Professional During the Postoperative Period
- Modifier 79 is a pricing modifier and should be reported in the first position.
- A new post-operative period begins when the unrelated procedure is billed.
Appropriate uses of CPT Modifier 79
• To describe an unrelated surgical procedure performed during the postoperative period of the original procedure by the same physician.
• When reporting identical procedures that are performed on the same day,
by the same physician, but are not the same service on the same
anatomical site.
Inappropriate uses of CPT Modfier 79
- The procedure performed is related to the original surgery or staged (anticipated) surgery.
- Placed on procedure codes with XXX indicator (global concept does not apply), in the global day field of the Medicare Physician’s Fee Schedule (MPFS) database.
- Reported on ambulatory surgical center (ASC) services.
- Note: If related to the original procedure, it is considered part of the global period.
CPT Modifier 80- Assistant Surgeon
- A physician, nurse practitioner, physician assistant or clinical nurse
specialist who is authorized to provide such services under state law can
serve as an assistant at surgery. - The “assistant at surgery” provides more than just ancillary services. The
operative note should clearly document the assistant surgeon’s role during
the operative session.
Facts
- Use the “80” modifier when the assistant at surgery service was provided by a physician.
- Use the “81” This modifier pertains to physician’s services only. Minimal surgical assistance may be identified by adding the modifier 81 to the usual procedure code and describes an assistant surgeon providing minimal assistance to the primary surgeon.
- Use the “82” modifier when a qualified resident surgeon is not available in a teaching facility:
- The unavailability of a qualified resident surgeon is a prerequisite for use of this modifier and the service must have been performed in a teaching facility.
- The circumstance explaining that a resident surgeon was not available must be documented in the medical record. This modifier is not intended for use by non-physician providers.
- Use the modifier “AS” for assistant at surgery services provided by a physician’s assistant (PA), nurse practitioner (NP), or clinical nurse specialist (CNS). The provider must accept the assignment.
CPT Modifier 81- Minimum Assistant Surgeon
Modifier 81 is appended to the procedure code for an assistant surgeon
who assists an operating or principal surgeon during part of a procedure.
Check the Medicare Physician Fee Schedule (MPFS) Indicator/Descriptor
Lists. Column A indicates if assistant at surgery is allowed.
Correct Use of CPT Modifier 81
- Append to appropriate code when more than one assistant is involved or if one person assists during a portion of surgery. Includes physicians providing minimal assistance to primary surgeon. Must be used with Type of Service 8 codes.
- This modifier identifies surgical assistant services
- Indicates exceptional medical circumstances exist
- Indicates primary surgeon has policy of never involving residents in preoperative, operative or postoperative care of his/her patients
CPT Modifier 82 – Assistant Surgeon (when qualified surgeon no available)
This modifier is used in the private insurance industry and is not commonly used in Medicare billing. Modifier 82 is only intended for use by physicians.
- This modifier is used when minimal surgical assistance is needed, but a qualified resident was not available (documentation required). First, check Medicare Physician Fee Schedule (MPFS) Indicator/Descriptor List. Column A indicates if assistant at surgery allowed/not allowed.
CPT Modifier 82 is used when:
- A qualified resident surgeon was not available to assist the primary surgeon
• The service was performed in a teaching facility
• Minimal surgical assistance was needed
• The primary surgeon has a policy of never involving residents in the care of
their patients
Modifier 82 is not intended for use by non-physicians assisting at surgery, such as
nurse practitioners or physician assistants. Documentation is required to support
the use of modifier 82.
Correct Use of CPT Modifier 82
- Physician:
- Assist-at-surgery allowed with appended modifiers 80, 81 or 82
- Allowed = 16% of surgery fee schedule allowable
- Modifier 82 needs a statement that “no qualified resident surgeon was available”
- Indicates exceptional medical circumstances exist
- Primary surgeon must have a policy of never involving residents in preoperative, operative or postoperative care of his/her patients
- Non Physician Practitioner (NPP) or mid-level practitioner (PA, NP, CNS):
- Append AS modifier only
- Allowed equals 85% of surgical assist or 16% allowable
Incorrect Use of CPT Modifier 82
- Inappropriate to bill physician assistant surgical services with AS modifier
- Inappropriate to append modifier 58 (staging) with any assistant surgery
CPT Modifier 90- Reference (Outside) Laboratory –(Referred tests)
Is used in medical coding to indicate that a laboratory procedure was performed by a party other than the treating or reporting physician. For example, a physician might order a CBC, draw blood, and send the specimen to an outside laboratory. The laboratory bills the physician for the service.
- • Modifier 90 is appended to a procedure code. The laboratory performing
the lab test must bill or submit the lab work directly.
• Modifier 90 indicates pass through billing
• A referring laboratory may bill for clinical laboratory tests on the clinical
laboratory fee schedule performed by a reference laboratory only if the
referring laboratory meets one of the following conditions:
• Located in, or is part of, a rural hospital
• Wholly owned by the entity performing such test. (referring laboratory
wholly owns the entity performing such test, or both the referring
laboratory and the entity performing such test are wholly-owned by a third
entity)
• Does not refer more than 30 percent of the clinical laboratory tests for
which it receives requests for testing during the year (not counting referrals
made under the wholly-owned condition described above)
Appropriate uses of CPT Modifier 90
- Only one laboratory may bill for a referred laboratory service.
- It is the responsibility of the referring laboratory to ensure that the reference laboratory does not bill Medicare for the referred service when the referring laboratory does.
- Referring laboratory may not bill in the event the reference laboratory bills or intends to bill Medicare.
Claim submission instructions
- Must include the referring and reference laboratory’s CLIA number.
- Laboratory testing require the presence of the referring and reference laboratory’s name and address.
- The reference laboratory for a service with a 90 modifier requires the performing provider’s information.
CPT Modifier 91- Repeat Clinical Diagnostic Laboratory Test
CPT Modifier 91 Is used to indicate that a laboratory test was repeated on the same day for the same patient. This modifier is used when multiple laboratory tests are needed during a patient’s treatment, such as repeat blood glucose tests.
You should not use modifier 91 for lab tests that are repeated to confirm initial results, due to equipment or specimen malfunctions, or when another one-time code is sufficient. Modifier 91 is different from modifier 59. Modifier 59 is used when the same test is performed on different sites. For example, if two wound cultures are taken from different sites, modifier 59 would be used. Modifier 91 is used to report any repeat clinical diagnostic laboratory test
being billed if:
- A single service (same CPT code) is ordered (for the same beneficiary)
- Specimen is collected more than once in a single day
- The service is medically necessary.
Appropriate Uses of CPT Modifier 91
To identify a subsequent medically necessary laboratory test on the same
day of the same previous laboratory test
Inappropriate Uses of CPT Modifier 91
When there are testing problems with the specimen a more appropriate procedure code is available to describe a series of test
- Rerun of a laboratory test is done to confirm results
- Testing problems with the equipment
- Procedure code describes a series of test
- For any reason when a normal one-time result is required
Claim Submission Instructions:
- Bill all services performed same day on the same claim
- Report each service on a separate line, with quantity of one and append 91 to the repeat procedure
- Documentation must support the use of the modifier
92-Alternative Laboratory Platform Testing
CPT Modifier 92 means that the laboratory testing is performed using a kit or transportable instrument that contains a single-use disposable analytical chamber. Modifier 92 is only used with HIV testing CPT codes 86701-86703.
For example, a patient might be tested for HIV using a hand-carried transportable kit. To obtain reimbursement for performing a rapid HIV test, providers can add modifier 92 to the usual laboratory procedure CPT code for the type of HIV test.
The general order of sequencing modifiers is: Pricing, Payment, Location.
Location modifiers are coded last in all coding situations
CPT Modifier 95 – Synchronous Telemedicine Service Rendered Via a Real-Time Interactive Audio and Video Telecommunication System
CPT Modifier 95 is used to indicate a synchronous telemedicine service, or a telehealth session. This means that the service was provided through a real time audio visual conference between a patient and a provider. The provider is at a different location from the patient.
The 95 modifier is only for codes listed in Appendix P of the CPT manual. Some insurance companies, such as Medicare, accept the 95 modifier. The 95 modifier can be used with a POS of 11 to indicate that the office visit was performed via telehealth. This allows the service to be paid at 100%. Using a POS of 02 subjects the code to a facility reduction of 15%
CPT Modifier 96 – Habilitative Services
Is used when the physical therapy services are rehabilitative in nature. The
CO, CQ, GO, and GP modifiers are all modifiers that indicate who performed the
service
CPT Modifier 97 – Rehabilitative Services
Is used to indicate that a service or procedure was provided for rehabilitative purposes. For example, a physician or other qualified healthcare professional might add modifier 97 to a physical therapy service code to indicate that the service was rehabilitative in nature.
The Affordable Care Act (ACA) requires coverage of certain essential health benefits (EHBs), including rehabilitative and habilitative services and devices. The Current Procedural Terminology (CPT®) code 97 is a medical procedural code under the range – Provider Services and Ambulatory Service Center Modifiers.
CPT Modifier 99- Multiple Modifiers
Append modifier 99 to a procedure or service as the first modifier when there are also two or more additional modifiers applicable to the service or procedure.
Master CPT Modifiers for Flawless Medical Coding
By understanding the significance of CPT modifiers and their appropriate application, medical coders can ensure accurate representation of services rendered, optimize billing practices, and contribute to a smooth healthcare revenue cycle. This guide provides a solid foundation for mastering CPT modifiers. Remember, staying current with coding guidelines and best practices is essential for coders to excel in this ever-evolving field.
Resources