Medical Coding Global Maternity Codes Are Being Eliminated in 2027: What Coders Need to Know
The American Medical Association (AMA) has approved a major overhaul of maternity care coding that will fundamentally change how obstetrical services are reported and reimbursed.
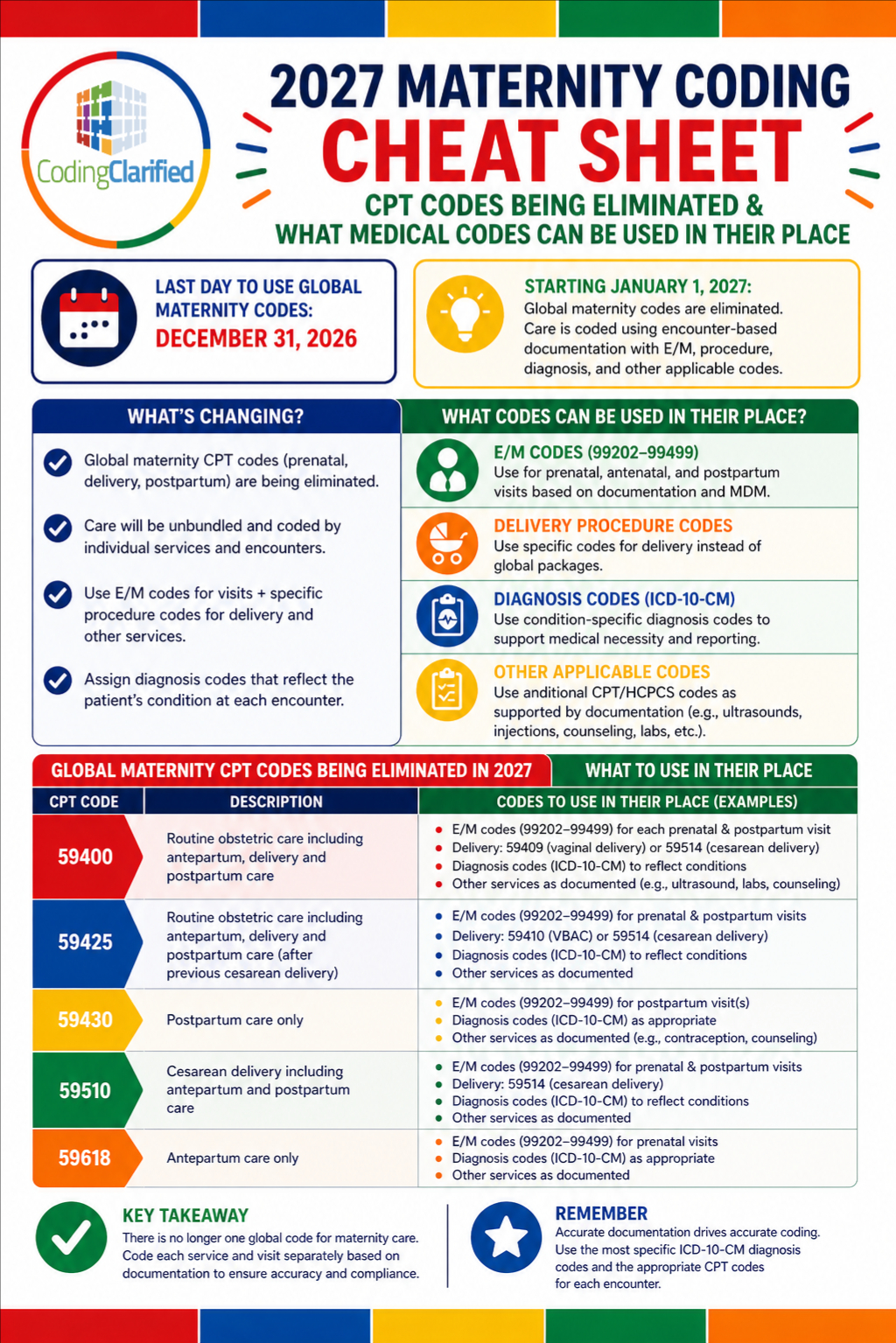
Effective January 1, 2027, traditional global maternity CPT® codes—such as 59400, 59510, 59610, 59425–59426—will be deleted and replaced with a fully unbundled, itemized billing model.
This is one of the most significant CPT® changes in years—and it will directly impact coding workflows, reimbursement, and documentation requirements.
What Is Changing?
1. Global Maternity Codes Are Being Eliminated
The long-standing “global OB package” will no longer exist.
Codes being removed include:
- 59400 – Vaginal delivery (global)
- 59510 – Cesarean delivery (global)
- 59610 – VBAC global care
- 59425–59426 – Antepartum bundled visits
A total of 16 obstetric codes will be deleted.
Why?
Organizations like American College of Obstetricians and Gynecologists (ACOG) determined that global codes no longer reflect modern maternity care, which now includes more screenings, counseling, and complex care management.
2. Shift to Unbundled (Itemized) Billing
Instead of one global code, providers will bill each service separately.
This includes:
- Each prenatal visit → E/M codes (99202–99499)
- Delivery → Delivery-only CPT codes (e.g., 59409, 59514)
- Postpartum visits → Separate E/M services
- Ancillary services → Billed individually (screenings, counseling, etc.)
ACOG recommends using the HCPCS modifier “TH” to identify pregnancy-related visits.
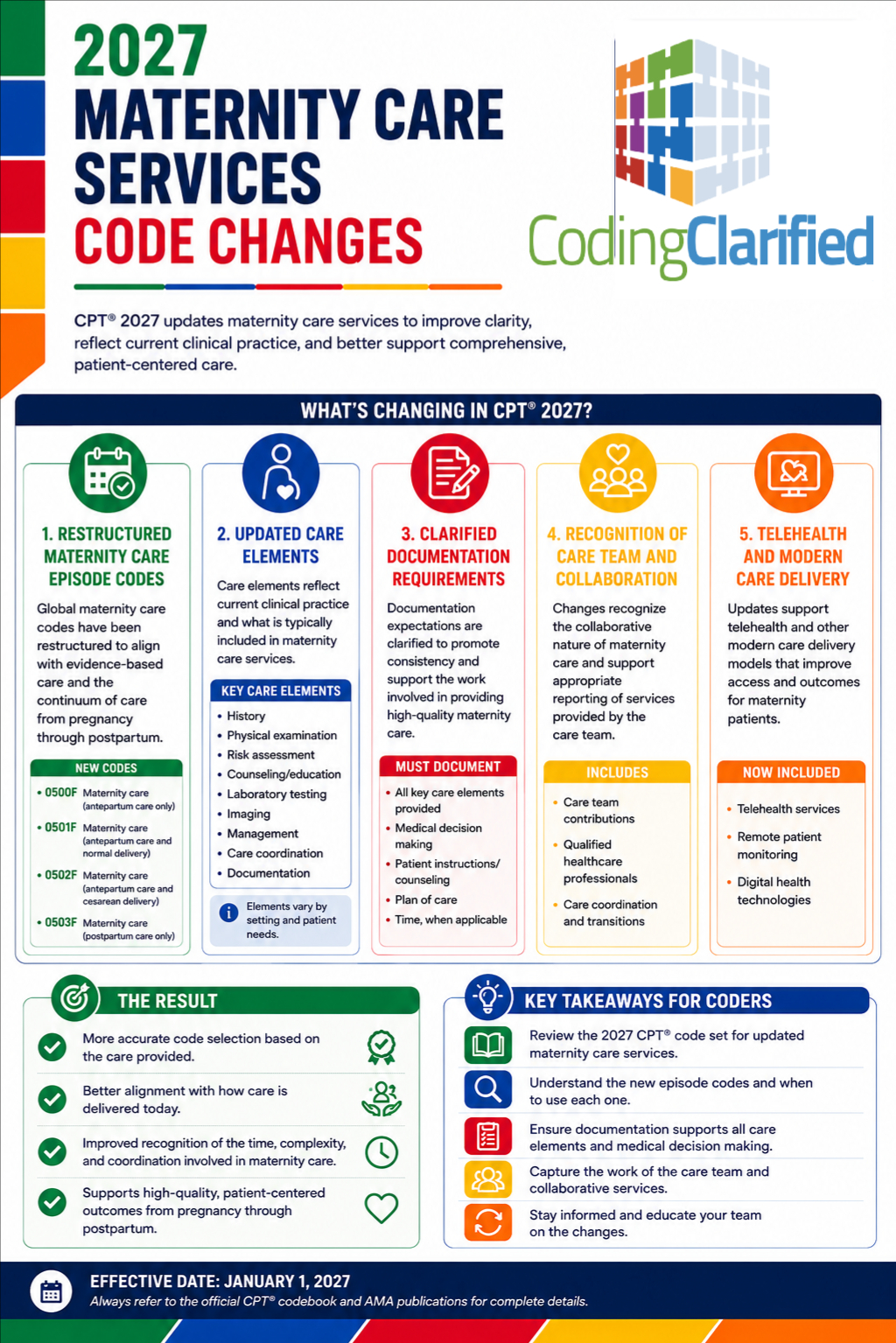
3. New CPT Code Structure Coming
- New maternity CPT codes (placeholder range 59XX1–59X12) will be introduced
- Existing codes will be revised
- Full details will be released closer to 2027
4. Delivery-Only Codes Will Remain
Not everything is going away.
These codes will still be used:
- 59409 – Vaginal delivery only
- 59514 – Cesarean delivery only
- 59612 / 59620 – VBAC delivery options
5. Labor Management May Use Inpatient E/M Codes
If labor spans multiple days or facilities:
- Use inpatient E/M codes (99221–99239)
This allows accurate billing when care is prolonged or shared across providers.
Why This Change Matters
Improved Data & Transparency
The new model allows payers to track:
- When pregnancy begins
- Frequency of visits
- Complications and outcomes
This improves care coordination and population health insights.
More Accurate Reimbursement
Under global billing:
- Many services were not separately reimbursed
Under unbundling:
- Providers can bill for:
- Mental health screenings
- Social determinants of health
- Genetic counseling
- High-risk monitoring
What This Means for Medical Coders & Billers
1. Increased Coding Volume
Instead of 1 global code per pregnancy, coders will now:
- Code every encounter separately
- Assign multiple CPT + ICD-10-CM codes
2. Documentation Will Be Critical
Each visit must support:
- Medical necessity
- E/M level selection
- Diagnoses addressed
- Time or MDM
Failure to document properly = denials or lost revenue
3. Higher Risk of Errors (and Opportunities)
More codes = more risk for:
- Undercoding
- Missed services
- Incorrect modifiers
But also more opportunity for:
- Accurate reimbursement
- Revenue capture
4. Workflow & System Changes
Practices will need to:
- Update EHR templates
- Train providers on documentation
- Adjust billing workflows
- Monitor payer-specific rules
What This Means for CPC Students
This change will directly impact exam preparation and real-world coding.
Key Takeaways for Students:
- Understand E/M coding deeply (this will be critical)
- Learn modifier usage (especially TH)
- Be comfortable coding:
- Prenatal visits
- Delivery services
- Postpartum care separately
Coding Guidelines & Tips
Tip 1: Master E/M Coding
E/M codes will replace most maternity visit reporting:
- Focus on MDM-based leveling
- Know time-based coding rules
Tip 2: Code Every Encounter Separately
Do NOT bundle services:
- Each visit = separate CPT code
- Each diagnosis must be linked correctly
Tip 3: Watch Modifier Usage
- TH modifier → Identifies maternity-related visits
- Other modifiers may apply based on payer rules
Tip 4: Track Trimester & Weeks of Gestation
Continue using ICD-10-CM codes:
- Z3A.XX (weeks of gestation)
- O codes (pregnancy complications)
These remain essential for risk adjustment and documentation.
Tip 5: Understand Split Care Scenarios
Different providers may bill:
- Prenatal care
- Delivery
- Postpartum care
Each provider bills only for services performed
Tip 6: Prepare for Payer Variability
Expect differences in:
- Medicaid vs commercial payers
- Modifier requirements
- Frequency limits
Coding Clarified Final Thoughts
The elimination of global maternity codes marks a major shift toward precision, transparency, and value-based care.
For medical coders, billers, and CPC students, this means:
- More detailed coding
- Greater reliance on E/M services
- Increased importance of documentation
- Expanded opportunities for accurate reimbursement
Those who adapt early and master these changes will be in a strong position as the industry transitions into this new model.