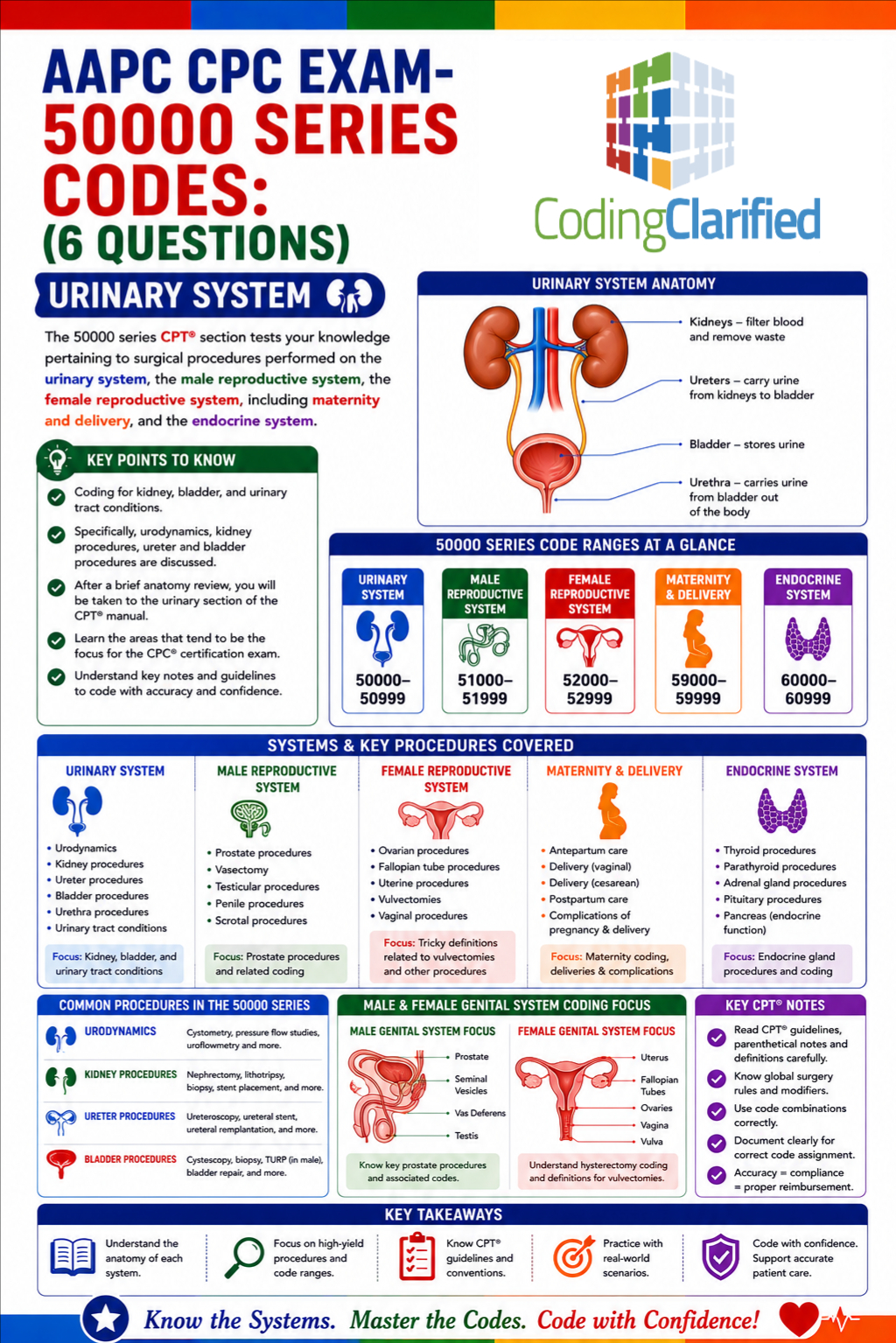
Medical Coding for Urology in 2026: CPT®, ICD-10-CM Updates, Guidelines, and CPC Tips
Author: Janine Mothershed CPC, CPC-I
Urology medical coding continues evolving rapidly in 2026 as healthcare organizations place greater emphasis on documentation specificity, outpatient surgical accuracy, payer compliance, and medical necessity validation. At the same time, minimally invasive procedures, robotic-assisted surgeries, and advanced diagnostic testing are becoming more common across urology specialty practices.
Because of these industry changes, coders must stay current on CPT®, ICD-10-CM, HCPCS Level II coding guidelines, modifier usage, and National Correct Coding Initiative (NCCI) edits. Otherwise, claim denials, compliance risks, and reimbursement delays can occur.
Additionally, urology coding requires a strong understanding of anatomy and operative terminology because many procedures involve the kidneys, bladder, ureters, prostate, urethra, and male reproductive system.
Whether you are preparing for the CPC exam, transitioning into specialty coding, or currently working in a urology practice, this guide explains the latest 2026 urology coding updates, documentation guidelines, coding tips, and compliance strategies.
Key Takeaway: Urology Coding in 2026
Urology coding in 2026 requires much more than simply selecting CPT® and ICD-10-CM codes. Instead, coders must understand anatomy, procedural intent, surgical approach, payer edits, modifier rules, and medical necessity documentation.
Furthermore, payers continue increasing audits related to:
- Modifier misuse
- Unspecified diagnoses
- Surgical bundling errors
- Medical necessity deficiencies
- Improper global surgery billing
Consequently, successful urology coders must carefully review operative reports, verify diagnosis specificity, understand NCCI edits, and remain updated on annual coding changes.
What Is Urology Medical Coding?
Urology medical coding involves translating physician documentation into standardized medical codes for billing, reimbursement, compliance, and statistical reporting.
Specifically, coders assign:
- CPT® procedure codes
- ICD-10-CM diagnosis codes
- HCPCS Level II codes
These codes represent conditions and services related to the urinary tract and male reproductive system.
Commonly coded urology conditions include:
- Benign prostatic hyperplasia (BPH)
- Kidney stones
- Hematuria
- Urinary tract infections (UTIs)
- Bladder cancer
- Prostate cancer
- Erectile dysfunction
- Hydronephrosis
- Overactive bladder
- Urinary incontinence
Meanwhile, common urology procedures include:
- Cystoscopy
- Lithotripsy
- Ureteroscopy
- TURP procedures
- Prostate biopsies
- Stent insertion
- Catheterization
- Robotic-assisted surgeries
Because many of these procedures involve bundled services and complex operative documentation, coders must pay close attention to detail.
2026 Urology Coding Updates and Trends
Increased Focus on Documentation Specificity
In 2026, insurance carriers and Medicare contractors continue emphasizing diagnosis specificity and documentation completeness. Therefore, vague documentation may trigger denials or payer audits.
For example, providers should clearly document:
- Acute versus chronic conditions
- Obstructed versus non-obstructed stones
- Right versus left side
- Presence of infection
- Severity or stage
- Complications
- Associated symptoms
Additionally, coders should avoid unspecified ICD-10-CM codes whenever more detailed documentation exists.
As a result, physician query processes remain extremely important in urology coding compliance workflows.
Expansion of Minimally Invasive Urology Procedures
At the same time, minimally invasive surgeries continue growing throughout urology practices in 2026. Consequently, coders must identify the exact surgical approach used during the procedure.
Operative reports may involve:
- Endoscopic approaches
- Percutaneous access
- Laser destruction
- Stone fragmentation
- Robotic-assisted surgery
- Diagnostic versus therapeutic interventions
Furthermore, coders should remember that robotic assistance itself is generally not separately billable. Instead, the primary CPT® code reflects the surgical service performed.
Modifier Audits Continue Increasing
Meanwhile, modifier audits remain a major compliance focus in 2026.
Commonly audited modifiers include:
- Modifier 25
- Modifier 57
- Modifier 59
- Modifier XS
- Modifier 51
- Modifier 24
Because modifier misuse can trigger recoupments and denials, coders should ensure documentation clearly supports separate and distinct procedural services.
Common Urology CPT® Codes in 2026
Cystoscopy CPT® Codes
Cystoscopy procedures remain among the most frequently coded services in urology.
| CPT® Code | Description |
|---|---|
| 52000 | Cystourethroscopy |
| 52204 | Cystoscopy with biopsy |
| 52224 | Cystoscopy with lesion or tumor removal |
| 52310 | Removal of ureteral stent |
| 52332 | Cystourethroscopy with ureteral stent insertion |
However, coders should always review CPT® parenthetical notes and NCCI edits before reporting multiple cystoscopy services together.
Additionally, fluoroscopy or imaging guidance may already be bundled into the primary procedure.
Prostate Procedure CPT® Codes
Because prostate disorders remain common in aging populations, prostate coding continues representing a significant portion of urology claims.
| CPT® Code | Description |
|---|---|
| 55700 | Prostate needle biopsy |
| 52601 | TURP procedure |
| 55866 | Laparoscopic radical prostatectomy |
| 76872 | Transrectal ultrasound |
Moreover, coders should carefully review whether pathology services, imaging guidance, or additional biopsies were separately documented.
Kidney Stone Procedure CPT® Codes
Kidney stone coding requires careful operative report review because similar procedures may involve entirely different CPT® codes.
| CPT® Code | Description |
|---|---|
| 50590 | Extracorporeal shock wave lithotripsy (ESWL) |
| 52352 | Ureteroscopy with stone extraction |
| 52353 | Ureteroscopy with lithotripsy |
| 50080 | Percutaneous nephrolithotomy |
Likewise, coders should verify whether ureteral stent placement occurred during the same operative session because bundling edits may apply.
Common ICD-10-CM Codes in Urology
Benign Prostatic Hyperplasia (BPH)
| ICD-10-CM Code | Description |
|---|---|
| N40.0 | BPH without lower urinary tract symptoms |
| N40.1 | BPH with lower urinary tract symptoms |
In many cases, additional symptom codes may also be necessary depending on payer policy and provider documentation.
Kidney Stones and Obstruction
Because kidney stone procedures are commonly audited, diagnosis specificity is especially important.
| ICD-10-CM Code | Description |
|---|---|
| N20.0 | Calculus of kidney |
| N20.1 | Calculus of ureter |
| N13.2 | Hydronephrosis with renal and ureteral calculous obstruction |
Furthermore, coders should determine whether obstruction, infection, or hydronephrosis is documented separately.
Urinary Tract Diagnoses
| ICD-10-CM Code | Description |
|---|---|
| N39.0 | Urinary tract infection |
| R31.0 | Gross hematuria |
| R31.9 | Hematuria, unspecified |
| N32.81 | Overactive bladder |
Nevertheless, coders should avoid separately reporting symptoms considered integral to the definitive diagnosis.
Important Urology Coding Guidelines
Always Review the Entire Operative Report
One of the most common urology coding mistakes occurs when coders rely only on the procedure title instead of reviewing the full operative report.
Instead, coders should review:
- Anatomical structures treated
- Surgical approach
- Scope insertion details
- Stone fragmentation methods
- Laser usage
- Stent insertion or removal
- Biopsy locations
- Catheter placement
Consequently, full operative note review significantly improves coding accuracy and compliance.
Understand NCCI Bundling Rules
NCCI edits frequently affect urology coding combinations. Therefore, coders should verify whether services are separately reportable.
For example:
- Diagnostic cystoscopy often bundles into surgical cystoscopy
- Catheterization may bundle into larger procedures
- Imaging guidance may already be included
- Stent placement edits may apply
As a result, coders should only append modifiers when documentation clearly supports separate services.
Verify Medical Necessity
Medical necessity continues representing one of the largest audit targets in 2026.
Accordingly, documentation should support:
- Symptoms
- Imaging findings
- Failed conservative treatment
- Diagnostic test results
- Physician assessment
- Surgical indication
Without sufficient medical necessity documentation, even correctly coded claims may deny.
Modifier Tips for Urology Coding
Modifier 25
Modifier 25 may apply when a significant and separately identifiable E/M service occurs on the same day as a minor procedure. In these situations, the provider documentation must clearly show work that goes beyond the standard preoperative evaluation associated with the procedure itself.
Modifier 57
When a provider makes the decision to perform a major surgery during an E/M encounter, modifier 57 may be appropriate. Unlike modifier 25, this modifier only applies to procedures that carry a 90-day global period.
Modifier 59
Coders use modifier 59 to identify separate and distinct procedural services. Before assigning it, however, the coder should determine whether a more specific X{EPSU} modifier better describes the circumstance.
Even so, coders should first determine whether another X{EPSU} modifier would be more appropriate.
Urology Coding Denial Prevention Tips
Match Diagnoses to Procedures Carefully
Diagnosis codes must support the medical necessity of the procedure performed.
For instance, stone removal procedures should correspond with documented urinary calculi diagnoses.
Monitor Global Surgery Rules
Many urology procedures include global periods. Therefore, postoperative visits may already be included in the surgical package.
Because of this, coders should review:
- Global periods
- Follow-up visit documentation
- Modifier requirements
- Surgical package guidelines
Verify Laterality
Laterality errors remain common in urology coding.
Consequently, coders should confirm:
- Right versus left side
- Bilateral involvement
- Multiple lesions
- Multiple stones
- Separate anatomical locations
Careful documentation review can significantly reduce denials related to anatomical specificity.
CPC Exam Tips for Urology Coding
Master Urology Anatomy
Strong anatomy knowledge is essential for both real-world coding and CPC exam success. Students should thoroughly understand kidney anatomy, ureter pathways, bladder anatomy, male reproductive structures, and urinary flow patterns. With a solid anatomy foundation, coders can identify CPT® procedures more accurately and navigate operative reports more efficiently.
Learn Common Operative Terminology
Urology operative terminology appears frequently on CPC certification exams. Terms such as lithotripsy, ureteroscopy, nephrostomy, fulguration, TURP, cystourethroscopy, and stent insertion should become familiar to every coding student. Because similar procedures may map to entirely different CPT® codes, understanding terminology is critical for accurate code selection.
Read CPT® Parenthetical Notes Carefully
Many important coding instructions appear directly beneath CPT® codes in the parenthetical notes. For this reason, students should carefully review add-on code instructions, modifier guidance, bundling edits, and separate procedure designations. Careful CPT® manual navigation not only improves exam performance but also strengthens coding accuracy in daily practice.
As a result, careful CPT® manual navigation can improve both exam performance and coding accuracy.
Common Urology Coding Mistakes
Coding From the Procedure Header Alone
Sometimes the procedure title does not reflect all services performed during surgery.
Therefore, coders should never code solely from the header.
Instead, reviewing the full operative report helps identify:
- Additional procedures
- Multiple treatment sites
- Bundled services
- Separate procedural work
Unbundling Included Services
Another common error involves separately coding services already included in the primary procedure.
For example:
- Diagnostic cystoscopy may bundle into surgical cystoscopy
- Fluoroscopy guidance may already be included
- Catheterization may bundle into major procedures
Consequently, coders should always review NCCI edits before assigning multiple CPT® codes.
Overusing Unspecified Diagnosis Codes
Although unspecified diagnosis codes are sometimes necessary, overuse may increase payer scrutiny and denial risk.
Accordingly, coders should query providers whenever documentation lacks specificity required for accurate ICD-10-CM reporting.
Additional Resources for Urology Medical Coding
For additional coding education and specialty coding resources, review these Coding Clarified articles:
- Medical Coding for Nephrology
- Acute on Chronic Kidney Failure Coding
- Telehealth Coding in 2026
- Pediatric Medical Coding and Billing in 2026
- CPC Exam Preparation Guide
Additionally, coders should routinely review guidance from:
Frequently Asked Questions About Urology Medical Coding
What is the most commonly coded urology procedure?
Cystoscopy procedures are among the most commonly coded urology services. However, kidney stone procedures, prostate surgeries, and ureteral stent placements are also extremely common.
What modifiers are commonly used in urology coding?
Common modifiers include modifier 25, modifier 57, modifier 59, modifier XS, and modifier 51. Nevertheless, coders should only append modifiers when documentation clearly supports separate procedural services.
Why are urology claims frequently denied?
Urology claims commonly deny because of:
- Insufficient medical necessity
- Modifier misuse
- Bundling errors
- Missing diagnosis specificity
- Incorrect laterality
- Global surgery billing issues
Therefore, careful documentation review is critical.
What is the difference between ureteroscopy and lithotripsy?
Ureteroscopy involves inserting a scope into the urinary tract to visualize or treat stones. Meanwhile, lithotripsy refers to stone fragmentation using laser or shock wave technology.
Because these procedures may occur together, coders must carefully review the operative report.
Why is anatomy important in urology coding?
Anatomy knowledge helps coders identify:
- Surgical approach
- Anatomical location
- Procedure intent
- Correct CPT® code selection
Additionally, anatomy questions appear frequently on the CPC exam.
Are robotic-assisted urology procedures separately billable?
In most cases, robotic assistance itself is not separately billable. Instead, coders report the primary surgical CPT® code representing the procedure performed.
What should CPC students focus on for urology coding?
CPC students should focus heavily on:
- Anatomy
- Operative terminology
- CPT® parenthetical notes
- Modifier rules
- NCCI edits
- Global surgery concepts
Because these topics appear frequently on certification exams, mastering them can improve testing confidence.
Final Thoughts on Urology Medical Coding in 2026
Successful urology coding in 2026 requires detailed documentation review, strong anatomy knowledge, modifier accuracy, and a thorough understanding of CPT® and ICD-10-CM guidelines. As minimally invasive procedures and specialty surgical techniques continue expanding, coders must stay current on payer policies, bundling edits, and medical necessity requirements.
Meanwhile, insurance audits remain heavily focused on diagnosis specificity, modifier usage, and surgical compliance. Coders who carefully review operative reports and validate documentation details can significantly improve reimbursement accuracy while reducing denial risk.
For CPC students, mastering urology terminology, anatomy, operative reports, and CPT® coding principles can strengthen both certification preparation and long-term career success.