Knee Replacement CPT Codes: 27447, 27446 & Revision Guide (2026)
By Janine Mothershed CPC, CPC-I
A complete 2026 guide for knee replacement coding. Learn the differences between total knee arthroplasty (27447), unicompartmental knee replacement (27446), and revision knee replacement codes (27486–27488). Includes ICD-10-CM coding, modifiers, documentation tips, CPC exam advice, and Medicare considerations.
Medical Coding for Knee Arthroplasty: CPT 27447, 27446, and Revision Rules
Key Takeaways
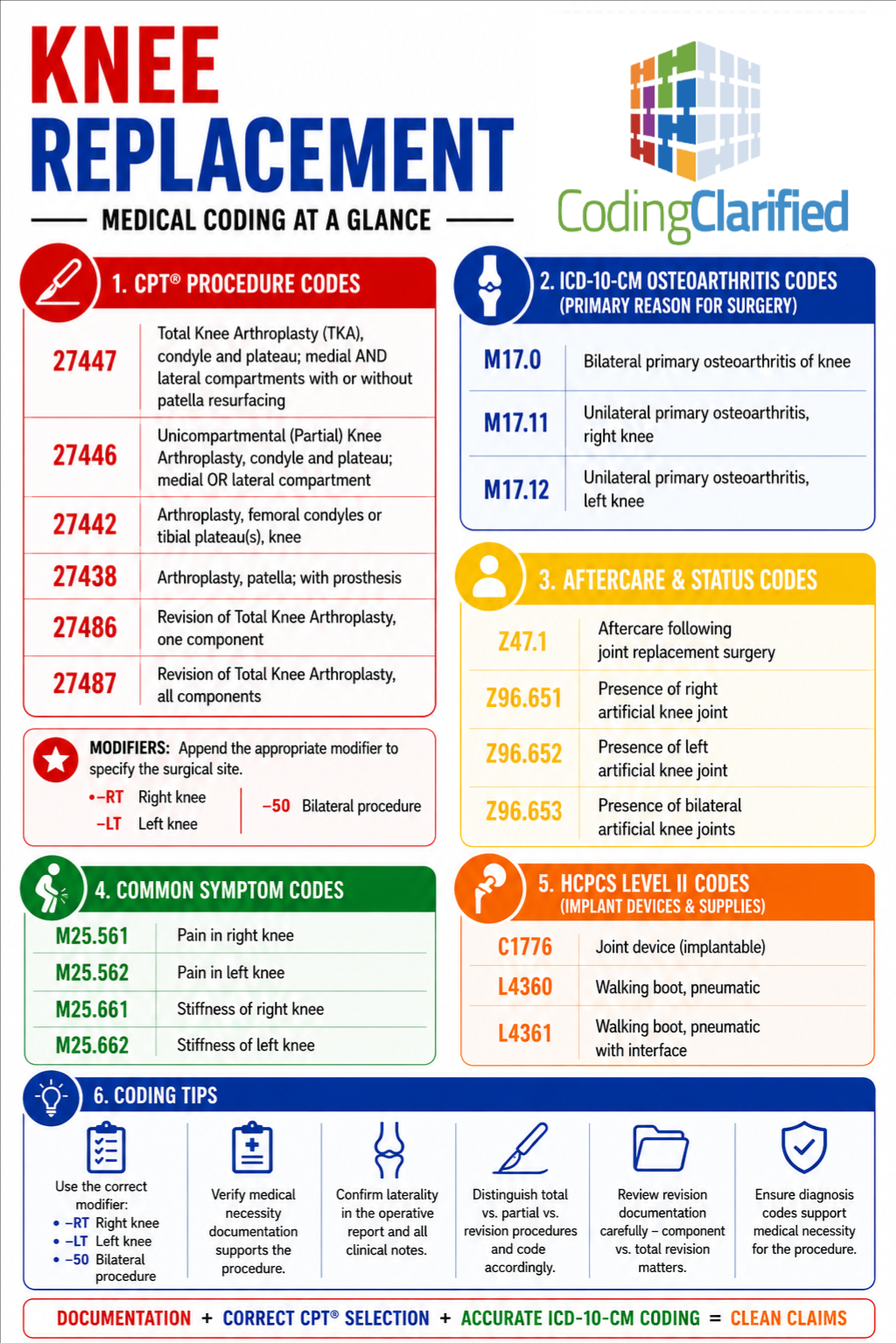
- CPT® 27447 reports total knee arthroplasty (TKA).
- CPT® 27446 reports unicompartmental (partial) knee replacement.
- Revision knee arthroplasty procedures are reported with CPT® 27486, 27487, or 27488 depending on the components revised or removed.
- Accurate coding requires proper documentation of the compartments involved and prosthetic components replaced.
- Laterality modifiers -LT and -RT remain essential for clean claim submission.
- Medical necessity should be supported by appropriate ICD-10-CM diagnoses such as M17.11, M17.12, or prosthetic complication codes.
- Medicare and commercial payers continue to closely monitor orthopedic claims in 2026.
Summary
What Is the CPT Code for a Knee Replacement?
The most commonly reported CPT code for a total knee replacement is 27447. A partial or unicompartmental knee replacement is reported with 27446. When a previously implanted prosthesis requires revision, coders typically report 27486 for a single component revision or 27487 for revision of both major components. Accurate reporting also requires proper diagnosis coding, laterality modifiers, and documentation of the surgical approach.
Quick Comparison: Knee Arthroplasty CPT Codes
| CPT Code | Procedure | Description |
|---|---|---|
| 27446 | Partial Knee Arthroplasty | Replacement of one compartment |
| 27447 | Total Knee Arthroplasty | Replacement of medial and lateral compartments |
| 27486 | Revision TKA | Revision of one component |
| 27487 | Revision TKA | Revision of femoral and tibial components |
| 27488 | Prosthesis Removal | Removal of knee prosthesis |
Why Knee Replacement Coding Matters in 2026
Today, total knee replacement remains one of the most commonly performed orthopedic procedures in the United States. As a result, payers continue to scrutinize documentation, medical necessity, and code selection.
Furthermore, Medicare Advantage plans and commercial insurers increasingly use preauthorization programs and claim edits to review orthopedic procedures. Therefore, accurate coding is more important than ever for both reimbursement and compliance.
According to guidance from the AAPC and CMS, coders should carefully review operative reports to determine whether the procedure was primary, partial, total, or revision surgery. Additionally, orthopedic surgery claims frequently undergo post-payment audits. Consequently, strong documentation and accurate code selection can help reduce denials, improve reimbursement, and support compliance efforts.
Authoritative References
Additionally, orthopedic surgery claims frequently undergo post-payment audits. Consequently, strong documentation and code selection can help reduce denials and recoupments.
Primary Knee Arthroplasty: Total vs. Partial
Understanding the distinction between total and partial knee replacement is one of the most important aspects of knee arthroplasty coding. While both procedures involve replacing damaged portions of the knee joint, they differ significantly in scope.
What Is a Total Knee Arthroplasty?
A total knee arthroplasty replaces the damaged articular surfaces of both the medial and lateral compartments of the knee. In many cases, the patella may also be resurfaced during the same procedure.
Because the entire joint is reconstructed, these procedures are typically performed when osteoarthritis affects multiple compartments. Consequently, patients who have severe joint degeneration often benefit from a total knee replacement rather than a partial procedure.
Furthermore, coders should carefully review the operative report to verify that multiple compartments were replaced before assigning CPT® 27447.
CPT Code for Total Knee Arthroplasty
CPT® 27447
Arthroplasty, knee, condyle and plateau; medial AND lateral compartments with or without patella resurfacing (total knee arthroplasty).
Common ICD-10-CM Diagnoses
- M17.0 Bilateral primary osteoarthritis of knee
- M17.11 Unilateral primary osteoarthritis, right knee
- M17.12 Unilateral primary osteoarthritis, left knee
- M17.31 Unilateral post-traumatic osteoarthritis, right knee
- M17.32 Unilateral post-traumatic osteoarthritis, left knee
Coding Example
A patient presents with severe tricompartmental osteoarthritis of the right knee. The surgeon replaces the femoral, tibial, and patellar articular surfaces.
Code Assignment
- 27447-RT
- M17.11
What Is a Partial Knee Replacement?
In contrast, a partial knee replacement replaces only one compartment of the knee. Rather than reconstructing the entire joint, the surgeon preserves the unaffected portions of the knee.
As a result, patients may experience shorter recovery times, less postoperative pain, and improved preservation of native anatomy.
Additionally, operative reports frequently use terms such as unicompartmental arthroplasty, medial compartment replacement, or lateral compartment replacement. Therefore, coders should become familiar with this terminology when reviewing orthopedic documentation.
CPT Code for Partial Knee Replacement
CPT® 27446
Arthroplasty, knee, condyle and plateau; medial OR lateral compartment.
Common Documentation Terms
Coders may encounter:
- Unicompartmental knee arthroplasty
- Medial compartment replacement
- Lateral compartment replacement
- Partial knee replacement
Coding Example
A patient undergoes replacement of only the medial compartment of the left knee.
Code Assignment
- 27446-LT
- M17.12
What About Patellofemoral Arthroplasty?
Coders frequently search for a dedicated CPT code for patellofemoral arthroplasty. However, CPT currently does not contain a specific code describing isolated patellofemoral replacement.
Therefore, providers may need to report an unlisted orthopedic procedure code when payer guidance supports its use. Nevertheless, coders should always verify payer-specific policies before reporting unlisted services because requirements vary considerably among carriers.
Revision Total Knee Arthroplasty Coding
Unlike primary knee replacements, revision procedures require a completely different coding approach.
Generally, revision surgery addresses failed prosthetic components caused by infection, loosening, instability, wear, fracture, or mechanical failure. As a result, documentation requirements are often more extensive than those for primary procedures.
Moreover, revision surgeries frequently involve greater physician work, additional operative time, and increased complexity. Therefore, accurate code selection becomes particularly important.
CPT 27486: Revision of One Component
Specifically, CPT® 27486 is used when only a single component of a previously implanted prosthesis is revised.
For example, the surgeon may replace only the tibial component while leaving the remaining prosthetic components intact. In this scenario, reporting CPT® 27486 would generally be appropriate.
Likewise, replacement of only the femoral component may also qualify for this code when supported by the operative report
Common Scenarios
- Tibial component revision only
- Femoral component revision only
- Patellar component revision only
Coding Example
A previously implanted tibial component becomes loose. The surgeon removes and replaces the tibial component while retaining the remaining prosthesis.
Code Assignment
- 27486
- T84.032A or T84.033A depending on laterality
CPT 27487: Revision of All Components
By comparison, CPT® 27487 is reported when both major prosthetic components are revised.
Typically, these procedures are more complex because the surgeon must remove multiple components and reconstruct the joint. Consequently, operative reports often contain significantly more detail regarding implant removal, bone preparation, and prosthetic reconstruction.
Furthermore, these procedures are frequently performed because of mechanical failure, loosening, or infection of the existing prosthesis.
Common Diagnoses
- T84.032A Mechanical loosening of internal right knee prosthetic joint
- T84.033A Mechanical loosening of internal left knee prosthetic joint
- T84.53XA Infection and inflammatory reaction due to internal knee prosthesis
Coding Example
The surgeon removes both femoral and tibial components due to prosthetic failure and replaces them with new components.
Code Assignment
- 27487
- Appropriate complication diagnosis code
CPT 27488: Removal of Prosthesis
CPT® 27488
Removal of prosthesis, including insertion of an antibiotic spacer when performed.
This code is commonly reported during staged treatment of infected prosthetic joints.
ICD-10-CM Coding for Knee Replacement Procedures
Likewise, diagnosis coding plays a critical role in supporting medical necessity.
The selected ICD-10-CM code should clearly explain why surgery was necessary. Additionally, diagnosis selection should match both physician documentation and operative findings.
Most importantly, coders should avoid assigning diagnoses that are not clearly documented within the medical record.
Osteoarthritis Diagnoses
- M17.0
- M17.11
- M17.12
- M17.31
- M17.32
Rheumatoid Arthritis Diagnoses
- M05.761
- M05.762
Prosthetic Joint Complications
- T84.032A
- T84.033A
- T84.53XA
Post-Traumatic Osteoarthritis
- M17.31
- M17.32
2026 Medicare Coverage Considerations
In 2026, Medicare continues to require documentation supporting medical necessity for knee replacement procedures.
Generally, documentation should demonstrate chronic pain, functional limitations, failed conservative treatment, and radiographic evidence of joint disease.
Additionally, Medicare Administrative Contractors (MACs) may publish Local Coverage Determinations (LCDs) that establish specific requirements.
Therefore, coders should review applicable payer policies before claim submission. Doing so can help reduce denials and improve reimbursement outcomes.
Modifier Considerations
Modifier selection remains an important component of orthopedic coding.
Commonly Used Modifiers
| Modifier | Description |
|---|---|
| -LT | Left side |
| -RT | Right side |
| -50 | Bilateral procedure |
| -22 | Increased procedural services |
| -59 | Distinct procedural service |
Nevertheless, modifier usage varies by payer. Therefore, coders should always review individual carrier requirements.
Documentation Requirements for Knee Arthroplasty Coding
Most importantly, accurate coding begins with complete physician documentation.
The operative report should clearly identify whether the procedure was total, partial, or revision arthroplasty. Additionally, the surgeon should document laterality, prosthetic components removed, components implanted, and any complications encountered during surgery.
Without this information, coders may struggle to support the reported CPT and ICD-10-CM codes. Consequently, claim denials and audit risks may increase.
The operative report should clearly identify:
- Total versus partial replacement
- Laterality
- Components removed
- Components implanted
- Revision versus primary procedure
- Prosthetic complications
- Medical necessity
- Surgical findings
Without these details, coders may struggle to support the reported procedure code.
Common Mistakes to Avoid
Unfortunately, even experienced orthopedic coders occasionally make mistakes.
Mistake #1: Confusing CPT 27446 and CPT 27447
First, determine whether one compartment or multiple compartments were replaced.
Mistake #2: Missing Laterality Modifiers
Second, always verify whether -LT or -RT should be appended.
Mistake #3: Using Revision Codes for Primary Procedures
Third, remember that revision codes apply only to previously implanted prosthetic joints.
Mistake #4: Selecting the Wrong Revision Code
Similarly, coders should carefully determine whether one component or multiple components were revised.
Mistake #5: Failing to Review Operative Reports
Furthermore, procedure titles alone do not always provide enough information for accurate code assignment.
Mistake #6: Assigning Unsupported Diagnosis Codes
Finally, ensure that all diagnosis codes support medical necessity and are documented by the provider.
CPC Student Tips
If you are preparing for the CPC® exam, knee arthroplasty coding is an area that deserves special attention.
First, highlight 27446 and 27447 in your CPT manual.
Next, create comparison notes for 27486, 27487, and 27488.
Additionally, focus on compartment terminology because exam questions frequently test this concept.
Moreover, practice reviewing operative reports rather than memorizing code descriptions alone.
Most importantly, understand the difference between primary and revision procedures. By doing so, you will be better prepared to answer orthopedic surgery questions accurately.
Study Strategies
- Highlight 27446 and 27447 in your CPT manual.
- Create comparison notes for 27486, 27487, and 27488.
- Focus on compartment terminology.
- Learn the difference between primary and revision procedures.
- Practice reviewing operative reports.
- Pay attention to laterality requirements.
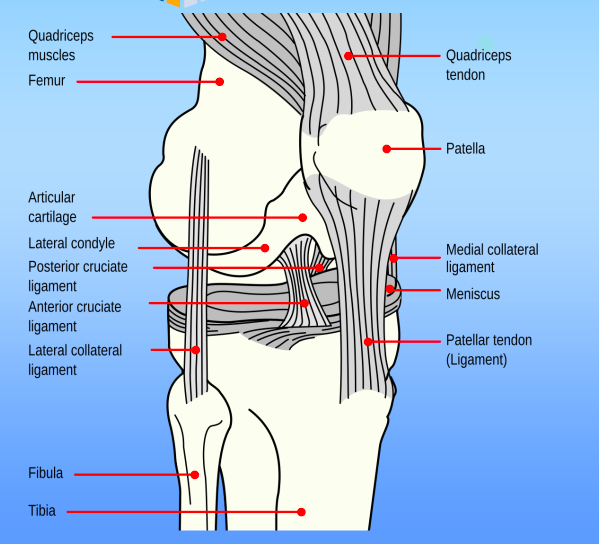
- Review musculoskeletal anatomy before tackling orthopedic coding questions.
Moreover, orthopedic surgery questions frequently contain distractor terminology. Therefore, careful reading is essential.
Related Coding Clarified Resources
Continue building your orthopedic coding knowledge with these related articles:
- Medical Coding orthopedics
- Medical Coding Fractures
- External Causes
- Medical Coding Global Surgery
- ICD-10 Codes for Pain: Chronic, Acute, and Cancer-Related (2026)
Browse our complete resource library
Frequently Asked Questions
What is the CPT code for a total knee replacement?
The most common CPT code for total knee arthroplasty is 27447.
What is the CPT code for a partial knee replacement?
A partial or unicompartmental knee replacement is reported with 27446.
What is the difference between CPT 27447 and CPT 27446?
27447 describes replacement of both medial and lateral compartments. Conversely, 27446 describes replacement of only one compartment.
What is CPT 27486 used for?
27486 is reported when a single component of a previously implanted knee prosthesis is revised.
When should CPT 27487 be reported?
Report 27487 when both major prosthetic components are revised during the same procedure.
What diagnosis codes are commonly used with total knee arthroplasty?
Common diagnoses include M17.11, M17.12, M17.31, and M17.32, depending on the documented condition.
Are laterality modifiers required for knee replacement procedures?
Most payers require -LT or -RT to identify the affected knee.
Is patella resurfacing separately reportable with CPT 27447?
No. Patella resurfacing is included in 27447 when performed as part of a total knee arthroplasty.
Coding Clarified Final Thoughts
Overall, knee arthroplasty coding requires careful analysis of physician documentation, operative reports, diagnosis selection, and payer requirements.
While CPT® 27447 remains the most frequently reported knee replacement code, coders must also understand when 27446, 27486, 27487, and 27488 apply.
Furthermore, accurate ICD-10-CM coding is essential for establishing medical necessity. Likewise, proper modifier usage can help prevent claim delays and denials.
Ultimately, thorough documentation, accurate code selection, and ongoing education will help coders improve reimbursement accuracy and maintain compliance throughout 2026.