
Medical Coding Foreign Body Guidelines and Practical Tips
Foreign body cases are common across emergency, outpatient, and surgical settings—and they’re also a frequent source of denials when coding guidelines aren’t followed. Accurate coding depends on location, intent, encounter type, documentation, and whether removal was performed. Below is a clear, coder-friendly breakdown of guidelines and tips to help you code foreign body cases correctly and confidently.
What Is Considered a Foreign Body?
A foreign body is any object that enters the body and does not naturally belong there. Examples include:
-
Glass, metal, wood, splinters
-
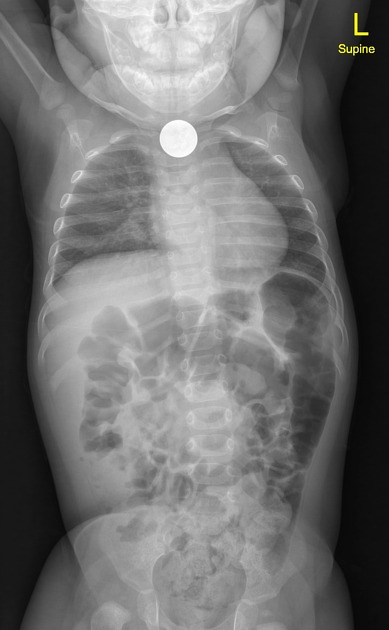
Coins, batteries, toys (common in pediatrics)
-
Food bolus impaction
-
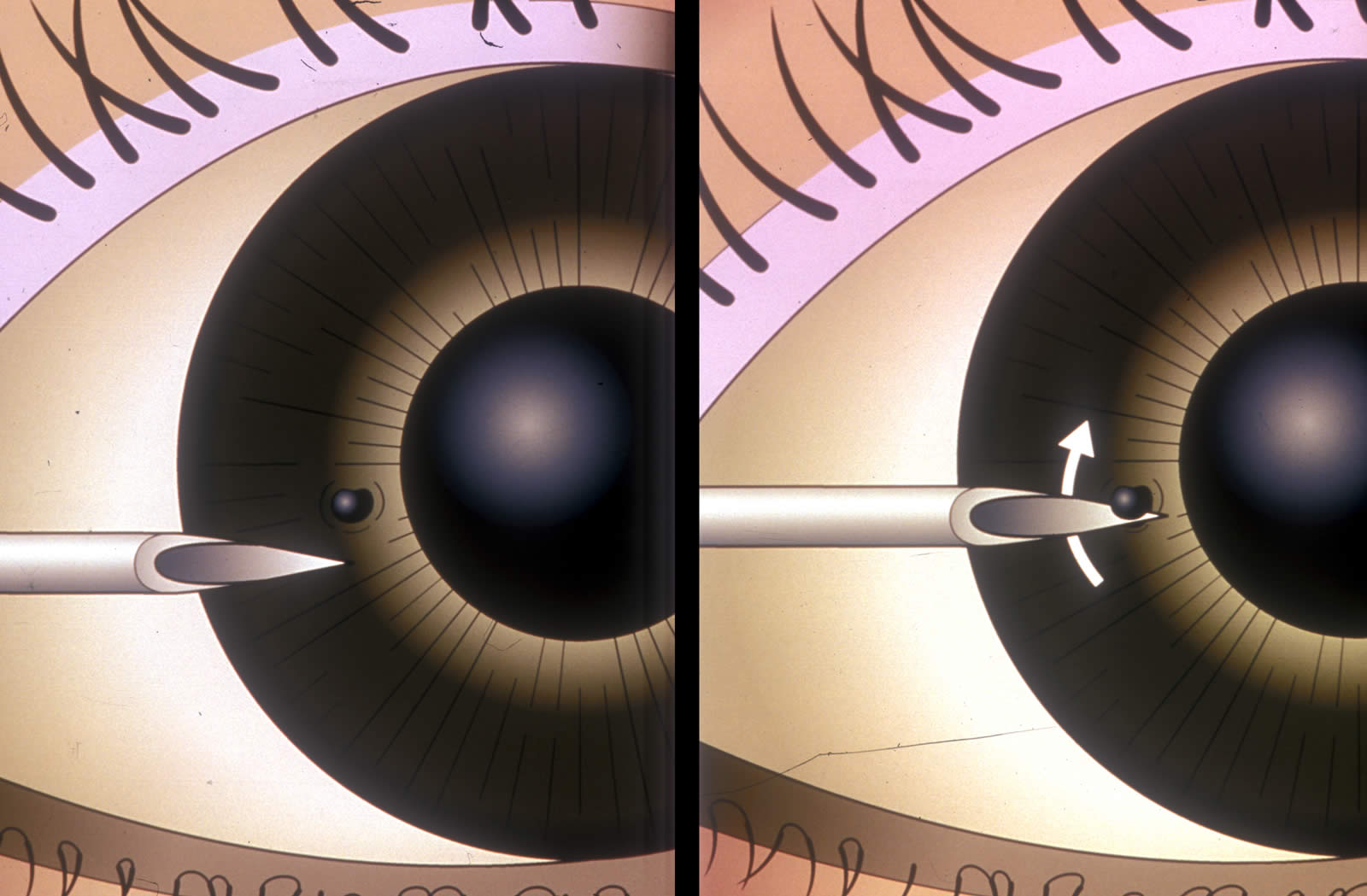
Contact lenses or debris in the eye
-
Retained surgical items
ICD-10-CM Diagnosis Coding Guidelines
Use the Correct Injury Chapter Code
Most foreign body diagnoses come from Chapter 19 (Injury, Poisoning, and Certain Other Consequences of External Causes) in ICD-10-CM.
Key points:
-
Select the code based on anatomical location
-
Choose the correct 7th character:
-
A – Initial encounter (active treatment)
-
D – Subsequent encounter
-
S – Sequela
-
Example:
-
Foreign body in right cornea, initial encounter → T15.01XA
Don’t Forget External Cause Codes (When Applicable)
External cause codes explain how the foreign body occurred.
Common external cause scenarios:
-
Accidental ingestion
-
Work-related injury
-
Household accident
Tips:
-
These codes are not mandatory for reimbursement, but are often required for:
-
Emergency department visits
-
Trauma cases
-
Pediatric encounters
-
State or payer-specific reporting
-
Always check payer and facility guidelines.
Document Intent Carefully
Intent affects code selection:
-
Accidental
-
Intentional self-harm
-
Assault
-
Undetermined
Never assume intent—use provider documentation only.
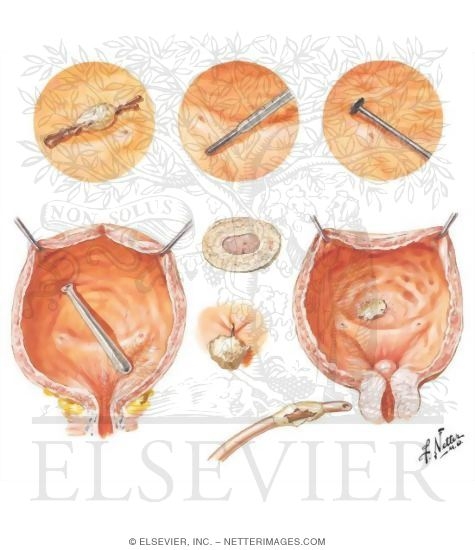
CPT Coding for Foreign Body Removal


Code Removal Only When Documented
A foreign body diagnosis code alone is not enough to bill a removal procedure.
To report a removal CPT code:
-
The provider must actively remove the object
-
Documentation must describe method, depth, and location
Examples from CPT:
-
Simple removal from skin → 10120
-
Complicated removal → 10121
-
Removal from ear or nose (varies by approach and complexity)
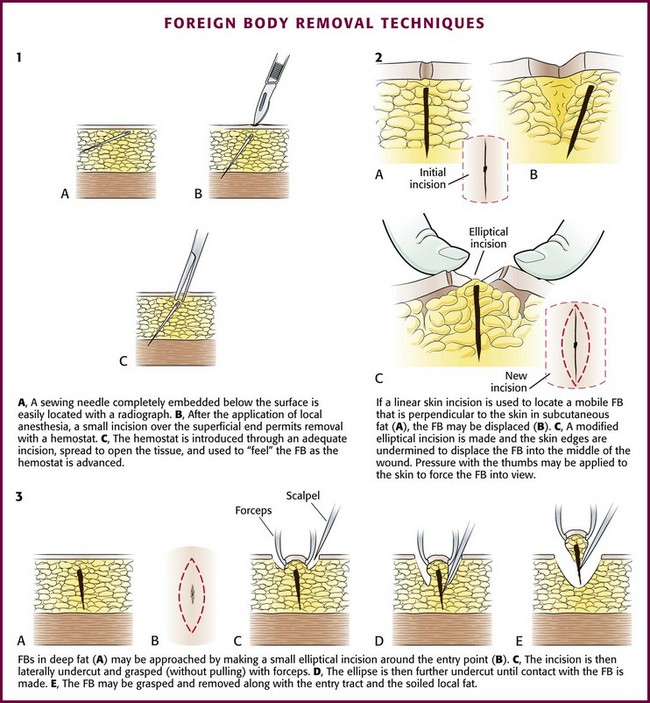
Simple vs. Complicated Matters
Coders must distinguish between:
-
Simple: superficial, minimal dissection
-
Complicated: deeper tissue, imaging guidance, layered closure, or extensive dissection
If complexity is unclear, query the provider.
E/M Services May Be Separately Reportable
An E/M visit may be billed in addition to foreign body removal if:
-
A significant, separately identifiable evaluation was performed
-
Proper documentation supports medical decision-making
Modifier -25 may be required.
AMA CPT® Evaluation and Management (E/M) Guidelines
Special Situations to Watch
Retained Surgical Foreign Bodies
-
Code as a complication, not a new injury
-
Often require combination codes or complication-specific sequencing
Foreign Body Without Removal
-
If the object is not removed, report:
-
The appropriate diagnosis code
-
Any imaging or observation services performed
-
-
Do not report a removal CPT code
Imaging Use
-
Imaging may support diagnosis or localization
-
Ensure documentation supports medical necessity
-
Follow bundling and modifier rules carefully
Common Coding Mistakes to Avoid
-
Reporting removal CPT codes without documentation
-
Using incorrect 7th characters
-
Omitting external cause codes when required
-
Assuming intent
-
Confusing simple vs. complicated removals
Pro Tips for Clean Claims
-
Always verify laterality
-
Match the diagnosis location with the procedure location
-
Review payer-specific policies
-
Query when documentation lacks detail
-
Confirm global period rules for minor procedures
Foreign body coding requires attention to detail, documentation, and intent. When guidelines are followed—and removal complexity is properly supported—claims are far more likely to process cleanly and withstand audits.