Chronic Obstructive Pulmonary Disease (COPD) Medical Coding Guide
Understanding Chronic Obstructive Pulmonary Disease (COPD)
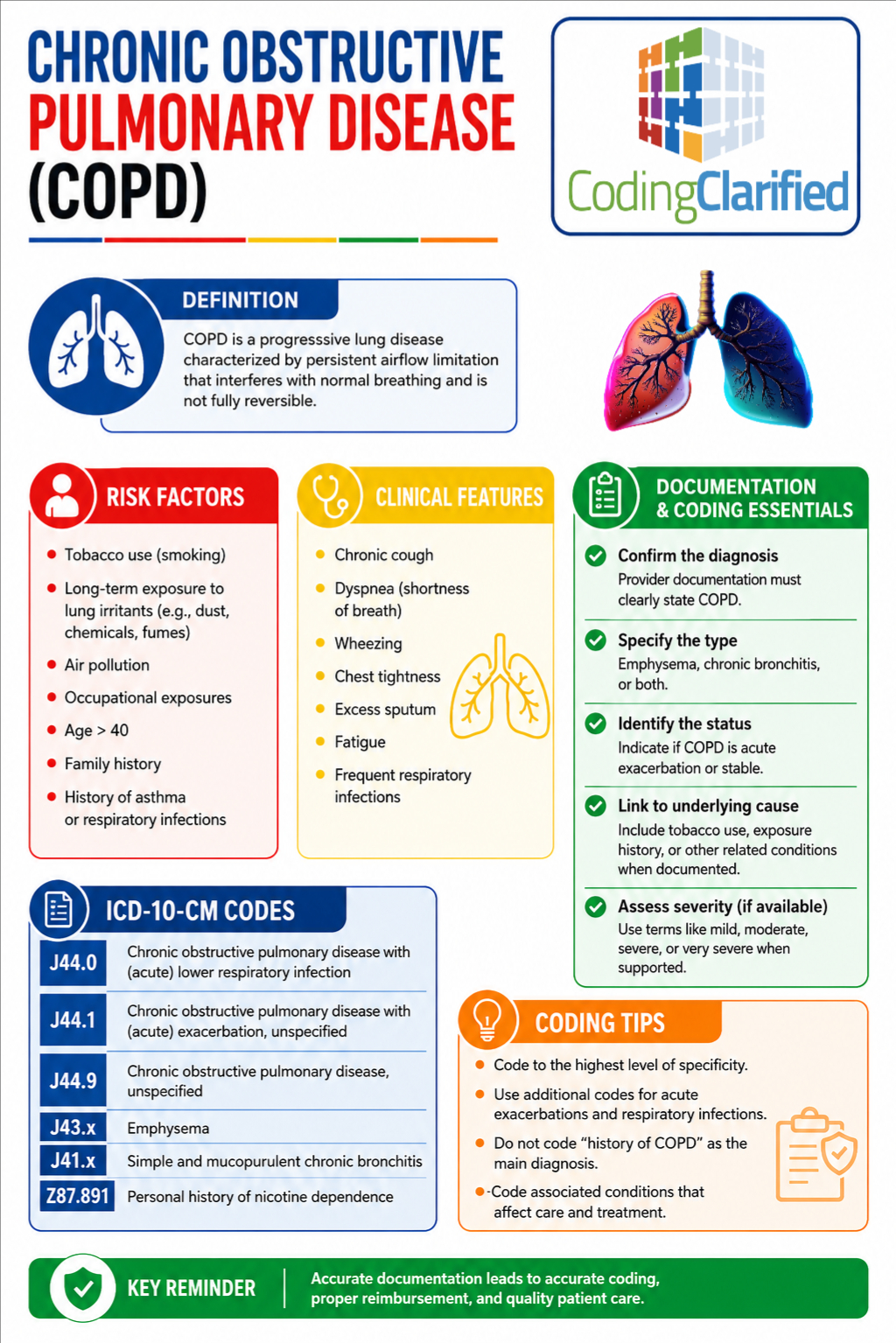
Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory disease that causes airflow limitation and breathing difficulties. Additionally, COPD is one of the most commonly coded chronic conditions in outpatient, inpatient, and risk adjustment coding environments. Because of its high prevalence and clinical complexity, medical coders must understand COPD documentation, ICD-10-CM guidelines, sequencing rules, and related complications.
Furthermore, COPD coding is frequently tested on the CPC exam because it requires coders to apply combination code guidelines, interpret physician documentation, and distinguish between acute and chronic respiratory conditions.
What Causes COPD?
COPD typically develops after long-term exposure to lung irritants. Common causes include:
- Cigarette smoking
- Secondhand smoke exposure
- Occupational chemical exposure
- Air pollution
- Genetic conditions such as alpha-1 antitrypsin deficiency
In many cases, providers document conditions such as chronic bronchitis, emphysema, or chronic airway obstruction under the COPD umbrella.
Common Symptoms of COPD
Patients with COPD may present with:
- Chronic cough
- Wheezing
- Dyspnea (shortness of breath)
- Excess mucus production
- Chest tightness
- Fatigue
- Frequent respiratory infections
Moreover, COPD symptoms often worsen during acute exacerbations, which significantly impacts coding and sequencing.
ICD-10-CM Coding for COPD
Main COPD ICD-10-CM Codes
| ICD-10-CM Code | Description |
|---|---|
| J44.0 | COPD with acute lower respiratory infection |
| J44.1 | COPD with acute exacerbation |
| J44.9 | COPD, unspecified |
| J43.9 | Emphysema, unspecified |
| J41.0-J42 | Chronic bronchitis categories |
COPD Coding Guidelines
1. COPD With Acute Exacerbation
When the provider documents COPD with acute exacerbation, assign:
- J44.1 — Chronic obstructive pulmonary disease with acute exacerbation
An exacerbation means the patient’s symptoms have suddenly worsened beyond baseline.
CPC Exam Tip
Do not confuse an exacerbation with an infection. An exacerbation alone does not automatically indicate pneumonia or bronchitis.
2. COPD With Acute Lower Respiratory Infection
If the provider documents COPD with an acute lower respiratory infection, assign:
- J44.0 first
- Then code the infection separately
Examples include:
- Pneumonia
- Acute bronchitis
- Influenza with respiratory involvement
Example
Provider Documentation:
COPD with acute bronchitis
Correct Coding:
- J44.0
- J20.9
Additionally, coders should always assign the secondary code to identify the infection.
3. COPD With Both Exacerbation and Infection
Sometimes documentation includes both an acute exacerbation and infection.
Example Documentation
COPD exacerbation due to pneumonia
Correct Coding
- J44.0
- J44.1
- Additional code for pneumonia
Therefore, both COPD combination codes may be required when supported by provider documentation.
Official ICD-10-CM Guideline Considerations
According to ICD-10-CM guidelines:
- COPD and asthma may both be coded if documented
- Acute respiratory failure may be sequenced first depending on circumstances of admission
- Tobacco use and dependence codes should also be assigned when documented
Tobacco Use Coding With COPD
Smoking history is extremely important in COPD coding.
Common tobacco-related codes include:
| Code | Description |
|---|---|
| F17.210 | Nicotine dependence, cigarettes, uncomplicated |
| Z87.891 | Personal history of nicotine dependence |
| Z72.0 | Tobacco use |
Coding Tip
Never assume active smoking unless documented by the provider.
COPD and Acute Respiratory Failure
Severe COPD cases may include respiratory failure.
Common codes include:
| Code | Description |
|---|---|
| J96.00 | Acute respiratory failure, unspecified whether with hypoxia or hypercapnia |
| J96.01 | Acute respiratory failure with hypoxia |
| J96.02 | Acute respiratory failure with hypercapnia |
However, sequencing depends on the reason for admission and provider documentation.
COPD Documentation Tips for Coders
Accurate coding begins with strong provider documentation. Therefore, coders should verify:
- Type of COPD
- Presence of acute exacerbation
- Presence of infection
- Tobacco use status
- Respiratory failure documentation
- Chronic bronchitis or emphysema specificity
- Oxygen dependence
- Mechanical ventilation status if applicable
Additionally, coders should review imaging reports, respiratory therapy documentation, discharge summaries, and physician progress notes for clarification opportunities.
Common COPD Coding Mistakes
Missing the Combination Code
One of the most common coding mistakes is assigning only the infection code without using J44.0.
Confusing Exacerbation With Infection
An exacerbation is not automatically an infection. The provider must document both conditions separately.
Forgetting Tobacco Codes
Smoking and tobacco dependence codes are often overlooked even though they may affect reimbursement, quality reporting, and risk adjustment.
Coding Unsupported Respiratory Failure
Coders should never assign respiratory failure solely based on oxygen use or abnormal lab values without provider documentation.
COPD and Risk Adjustment (HCC Coding)
COPD is also important in Hierarchical Condition Category (HCC) coding because it impacts risk scores and reimbursement models.
Furthermore, chronic pulmonary disease diagnoses may affect:
- Medicare Advantage RAF scores
- Quality measures
- Chronic condition management programs
Because of this, accurate documentation specificity is essential.
COPD CPC Exam Preparation Tips
COPD coding frequently appears on the CPC exam. Therefore, students should focus on:
Learn Combination Codes
Understand when:
- J44.0
- J44.1
- J44.9
should be assigned individually or together.
Read Documentation Carefully
The CPC exam often tests subtle wording differences such as:
- “with”
- “due to”
- “acute”
- “chronic”
- “exacerbation”
Consequently, missing one word can change code assignment entirely.
Practice Sequencing
Know when:
- respiratory failure
- pneumonia
- COPD exacerbation
should be listed first.
Review Respiratory Chapter Guidelines
The respiratory chapter contains many combination coding rules that CPC students should memorize.
Real-World COPD Coding Scenario
Example Case
Documentation
Patient admitted with COPD exacerbation and acute pneumonia. History of nicotine dependence.
Correct ICD-10-CM Coding
- J44.0 — COPD with acute lower respiratory infection
- J44.1 — COPD with acute exacerbation
- J18.9 — Pneumonia, unspecified organism
- F17.210 — Nicotine dependence, cigarettes, uncomplicated
This type of scenario is extremely common on CPC exams and in production coding environments.
COPD Medical Coding Summary
Chronic Obstructive Pulmonary Disease (COPD) coding requires careful attention to provider documentation, ICD-10-CM combination coding rules, sequencing guidelines, and respiratory complications. Additionally, coders must distinguish between exacerbations, infections, respiratory failure, and chronic tobacco use documentation.
Because COPD is frequently seen in hospitals, physician offices, emergency departments, and risk adjustment coding, mastering these guidelines is essential for both CPC exam success and real-world coding accuracy.
Ultimately, strong COPD coding skills help improve:
- Coding accuracy
- Reimbursement
- Compliance
- Risk adjustment reporting
- Patient record integrity
By understanding COPD coding guidelines and practicing respiratory coding scenarios regularly, CPC students and professional coders can build confidence and improve coding performance.