Ethmoidectomy and Maxillary Antrostomy Medical Coding Guide (2026 CPC Review)
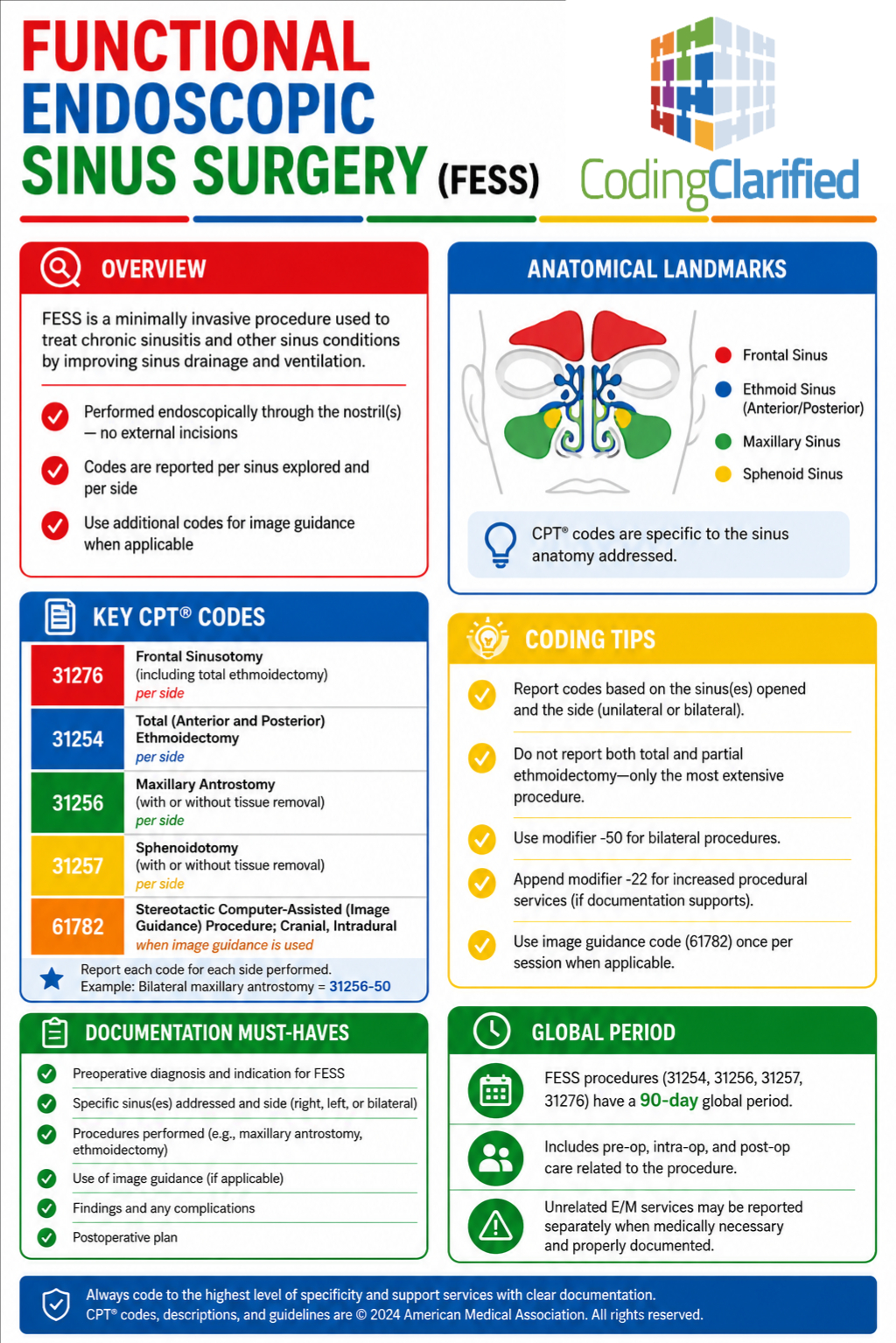
Functional Endoscopic Sinus Surgery (FESS): CPT®, ICD-10-CM, and Coding Rationales
Chronic sinusitis is one of the most frequently coded conditions in otolaryngology and outpatient surgery settings. Therefore, medical coders must understand how to accurately code Functional endoscopic sinus surgery (FESS) procedures. In this operative report, the physician performed a left anterior ethmoidectomy and a left maxillary antrostomy to treat chronic sinusitis and sinus cephalgia. Additionally, the surgeon widened the maxillary ostium and removed diseased tissue from the ethmoid region.
Because FESS procedures involve multiple sinus cavities and bundled endoscopic services, coders must review the operative documentation carefully. Furthermore, CPC students should pay close attention to anatomy terminology, tissue removal language, laterality, and sinus-specific operative findings. As a result, understanding these details can significantly improve coding accuracy on both the CPC exam and real-world surgical cases.
Key Takeaway for CPC Students
For this operative report:
- CPT® 31254 is reported for the left anterior ethmoidectomy
- CPT® 31256 is reported for the left maxillary antrostomy
- ICD-10-CM chronic sinusitis codes are assigned based on the sinus cavities treated
- Sinus cephalgia may support additional symptom coding when payer guidelines allow
- Careful operative note review is essential for accurate FESS coding
Most importantly, coders should never rely solely on the procedure title when assigning CPT® codes. Instead, reviewing the body of the operative report is critical for identifying the exact sinus structures treated.
Medical Coding Scenario
Medical Specialty
Allergy / Immunology
Procedure Description
The patient underwent Functional Endoscopic Sinus Surgery (FESS), including:
- Left anterior ethmoidectomy
- Left maxillary antrostomy
- Widening of the maxillary ostium
- Scar tissue removal
- Endoscopic sinus evaluation
In addition, the physician inspected the right nasal cavity; however, no right-sided surgical procedure was performed.
Preoperative Diagnoses
- Chronic sinusitis
- Sinus cephalgia
Postoperative Diagnoses
- Chronic sinusitis
- Sinus cephalgia
Important Operative Report Findings
| Operative Finding | Coding Importance |
|---|---|
| Chronic inflammation in left maxillary sinus | Supports chronic maxillary sinusitis diagnosis |
| Ethmoid cells opened and removed | Supports ethmoidectomy coding |
| Natural maxillary ostium widened | Supports maxillary antrostomy coding |
| Scar tissue removed | Supports tissue removal documentation |
| Endoscopic sinus surgery performed | Indicates FESS procedure family |
| Left-sided intervention only | Supports LT modifier usage |
| Right side inspected only | No right-sided procedure coded |
CPT® Coding
Final CPT® Code Assignment
| CPT® Code | Description |
|---|---|
| 31254-LT | Nasal/sinus endoscopy with partial (anterior) ethmoidectomy |
| 31256-LT | Nasal/sinus endoscopy with maxillary antrostomy |
CPT® Coding Rationales
CPT® 31254 — Anterior Ethmoidectomy
According to the operative report, the physician entered and removed diseased anterior ethmoid cells endoscopically. Specifically, the documentation states:
- “The ethmoid bone was then entered”
- “Anterior ethmoid cells were entered”
- “Inferior ethmoid cells were taken down”
Because the procedure involved only the anterior ethmoid region, CPT® 31254 is appropriate. In contrast, CPT® 31255 would require documentation supporting a total ethmoidectomy involving both anterior and posterior ethmoid cells.
Additionally, coders should remember that the ethmoid sinus is divided into multiple air cells. Consequently, identifying whether the surgeon treated anterior versus total ethmoid disease is extremely important for CPT® selection.
CPT® 31256 — Maxillary Antrostomy
During the procedure, the physician localized and widened the natural maxillary ostium. Furthermore, the surgeon removed scar tissue using forceps and a microdebrider. As a result, the operative documentation supports a maxillary antrostomy performed endoscopically.
The operative report also states:
- “The natural maxillary ostium was localized”
- “The ostium was widened”
- “Scar tissue was taken down”
Because tissue removal occurred, CPT® 31256 is supported. Therefore, coders should carefully review operative language describing debridement, tissue removal, or scar excision during FESS procedures.
ICD-10-CM Coding
Final ICD-10-CM Code Assignment
| ICD-10-CM Code | Description |
|---|---|
| J32.0 | Chronic maxillary sinusitis |
| J32.2 | Chronic ethmoidal sinusitis |
| R51.9 | Headache / sinus cephalgia |
ICD-10-CM Coding Rationales
J32.0 — Chronic Maxillary Sinusitis
CT findings demonstrated chronic inflammation involving the left maxillary sinus. Additionally, the physician documented obstruction involving the maxillary ostium and chronic sinus disease. Because the surgeon treated the maxillary sinus directly during the procedure, J32.0 is supported by the documentation.
Moreover, coders should always confirm whether the operative findings support chronic rather than acute sinusitis before assigning ICD-10-CM codes.
J32.2 — Chronic Ethmoidal Sinusitis
During surgery, the physician entered and removed diseased anterior ethmoid cells. Consequently, chronic ethmoidal sinusitis may also be assigned when supported by provider documentation and payer-specific guidelines.
Furthermore, coders should connect operative findings with the documented diagnoses to ensure medical necessity is clearly supported.
R51.9 — Sinus Cephalgia
Both the preoperative and postoperative diagnoses documented sinus cephalgia. Since cephalgia means headache, coders may assign R51.9 when payer edits allow separate symptom reporting.
However, coding professionals should always review payer-specific rules before separately reporting symptoms associated with definitive diagnoses.
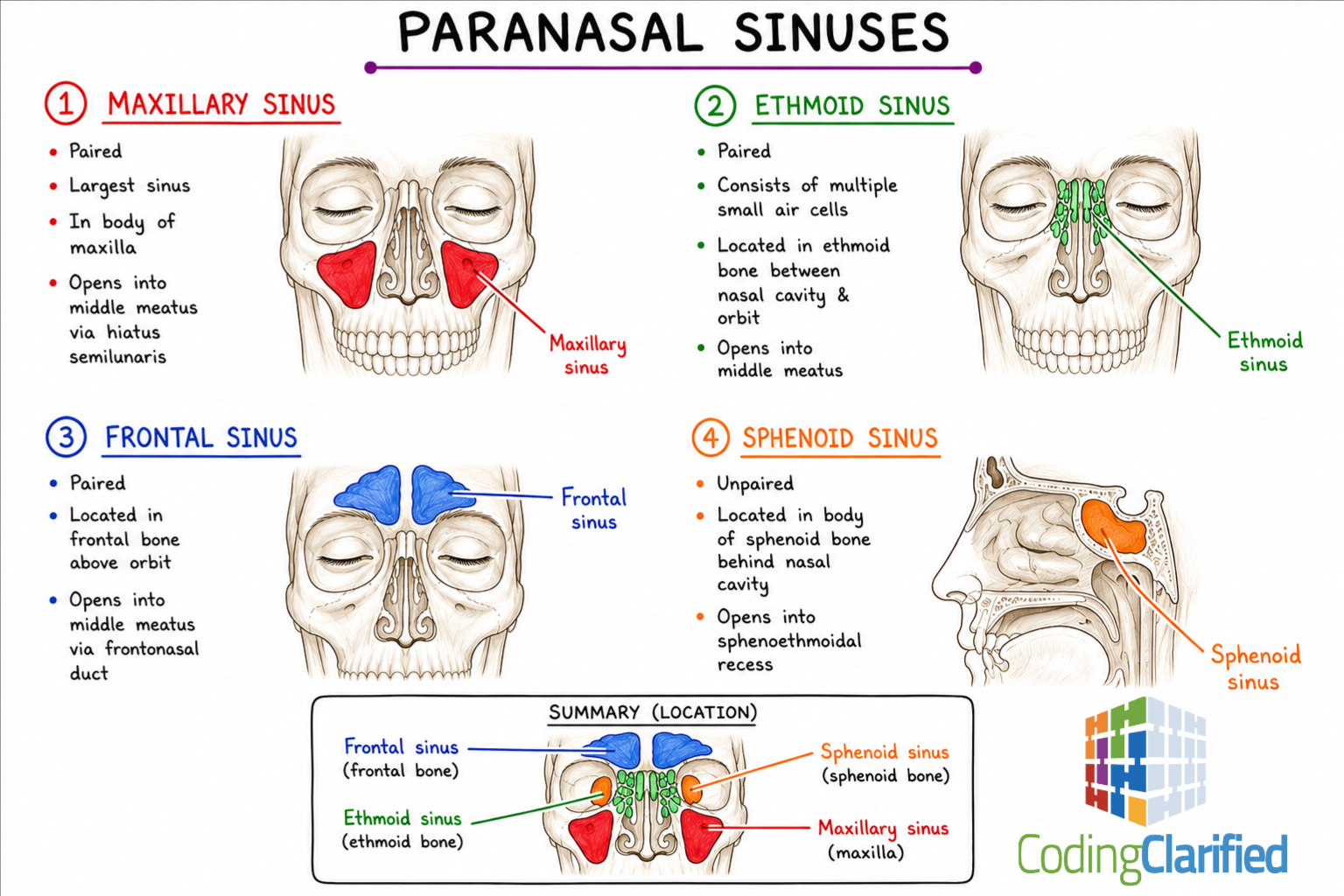
Anatomy Review for CPC Students
Understanding sinus anatomy is critical for accurate FESS coding. Therefore, CPC students should become familiar with the following sinus cavities:
- Maxillary sinus
- Ethmoid sinus
- Frontal sinus
- Sphenoid sinus
Additionally, coders should understand the location of the maxillary ostium and ethmoid air cells because these structures are commonly referenced in operative reports.
Without strong anatomy knowledge, sinus surgery coding becomes much more difficult. Consequently, anatomy review remains one of the best ways to improve coding accuracy and CPC exam performance.
Operative Note Breakdown
Evidence Supporting Ethmoidectomy
The surgeon documented:
“Anterior ethmoid cells were entered”
and
“Inferior ethmoid cells were taken down”
Accordingly, this documentation directly supports ethmoidectomy coding.
Evidence Supporting Maxillary Antrostomy
The operative report states:
“The natural maxillary ostium was localized”
and
“The ostium was widened”
Therefore, this documentation supports maxillary antrostomy coding.
FESS Coding Guidelines and Tips
1. Review the Entire Operative Report
Rather than coding directly from the procedure title, coders should carefully review the body of the operative report. For example, sinus anatomy and tissue removal details are often buried within the procedural description.
As a result, reading the full operative note helps prevent incorrect CPT® code assignment.
2. Watch for Bundled Procedures
Many sinus surgery services are bundled together under FESS coding guidelines. For instance:
- Diagnostic sinusoscopy is included within the surgical endoscopy
- Surgical approaches are included
- Nasal packing placement is generally not separately reportable
Because bundling edits are common in sinus surgery coding, coders should review National Correct Coding Initiative (NCCI) edits carefully.
3. Identify the Exact Sinus Treated
Each sinus cavity has different CPT® coding options. Therefore, coders must determine whether the physician treated the:
- Maxillary sinus
- Ethmoid sinus
- Frontal sinus
- Sphenoid sinus
Most importantly, accurate code selection depends on identifying the exact sinus region involved.
4. Determine Whether Tissue Was Removed
Another common CPC exam trap involves tissue removal documentation. In many FESS procedures, the presence or absence of tissue removal changes code selection significantly.
For example:
- CPT® 31256 includes tissue removal
- CPT® 31267 may apply when more extensive tissue removal is documented
Accordingly, coders should always compare the operative details against the CPT® descriptors before finalizing code assignment.
Common Coding Mistakes
| Common Error | Why It Is Incorrect |
|---|---|
| Coding bilateral procedures | Only the left side was treated |
| Reporting diagnostic endoscopy separately | Included in surgical endoscopy |
| Missing the ethmoidectomy | Ethmoid cells were clearly removed |
| Assigning acute sinusitis codes | Documentation supports chronic sinusitis |
| Coding the right side | Right side was inspected only |
Modifier Tip
Because the procedures were performed on the left side only, the LT modifier is appropriate when required by payer guidelines.
Additionally, coders should always review payer-specific modifier requirements before claim submission.
Anesthesia Coding Tip
Initially, the patient received IV sedation. However, the procedure was converted to general endotracheal anesthesia because of anticipated bleeding and airway concerns.
Nevertheless, anesthesia services are not separately coded by the procedural coder unless anesthesia coding responsibilities are specifically assigned.
Medical Necessity Considerations
Several factors support medical necessity in this case, including:
- Chronic facial pain
- Chronic sinus inflammation
- Obstructed maxillary ostium
- Persistent sinus symptoms
- Failed prior sinus surgery
- CT-confirmed sinus disease
Furthermore, the patient’s previous surgical history and ongoing symptoms support the need for additional surgical intervention.
CPC Exam Strategies
When coding sinus surgery cases on the CPC exam, students should:
- Highlight anatomy references
- Circle tissue removal terminology
- Identify laterality
- Review bundling guidelines
- Compare operative details to CPT® descriptors
In addition, students should avoid coding directly from the procedure heading alone. Instead, successful coders carefully analyze the operative narrative line-by-line.
Final CPC Review Summary
Overall, this operative report demonstrates a classic Functional Endoscopic Sinus Surgery (FESS) coding scenario commonly tested on CPC exams. Because sinus surgery coding involves anatomy, operative technique, tissue removal, and bundling principles, coders must analyze the documentation carefully.
In particular, CPC students should focus on:
- Distinguishing anterior versus total ethmoidectomy
- Identifying maxillary antrostomy documentation
- Recognizing tissue removal terminology
- Applying chronic sinusitis ICD-10-CM guidelines
- Reviewing sinus anatomy thoroughly
Ultimately, accurate sinus surgery coding requires much more than reading the procedure title alone. Instead, successful coders connect anatomy, operative findings, and CPT® descriptors to assign the most accurate codes possible.