
Medical Coding and Billing for X-Rays in 2026: CPT Codes, Modifiers, Documentation, and Reimbursement Guidelines
Author: Janine Mothershed CPC, CPC-I
Radiology services remain among the most frequently reported diagnostic procedures in healthcare. Whether performed in physician offices, urgent care centers, emergency departments, or hospitals, X-rays require accurate coding, proper documentation, and correct modifier usage to ensure compliant billing and optimal reimbursement. Moreover, as payer scrutiny continues to increase, coding professionals must pay close attention to documentation details. As a result, even minor coding errors can lead to denials, delayed payments, or compliance concerns.
As we move through 2026, payers continue to scrutinize radiology claims for medical necessity, component billing errors, and documentation deficiencies. Consequently, coders must understand not only the appropriate CPT® codes but also Medicare requirements, National Correct Coding Initiative (NCCI) edits, and payer-specific billing rules.
This guide explains everything medical coders, billers, and CPC students need to know about coding and billing X-rays in 2026.
Key Takeaways
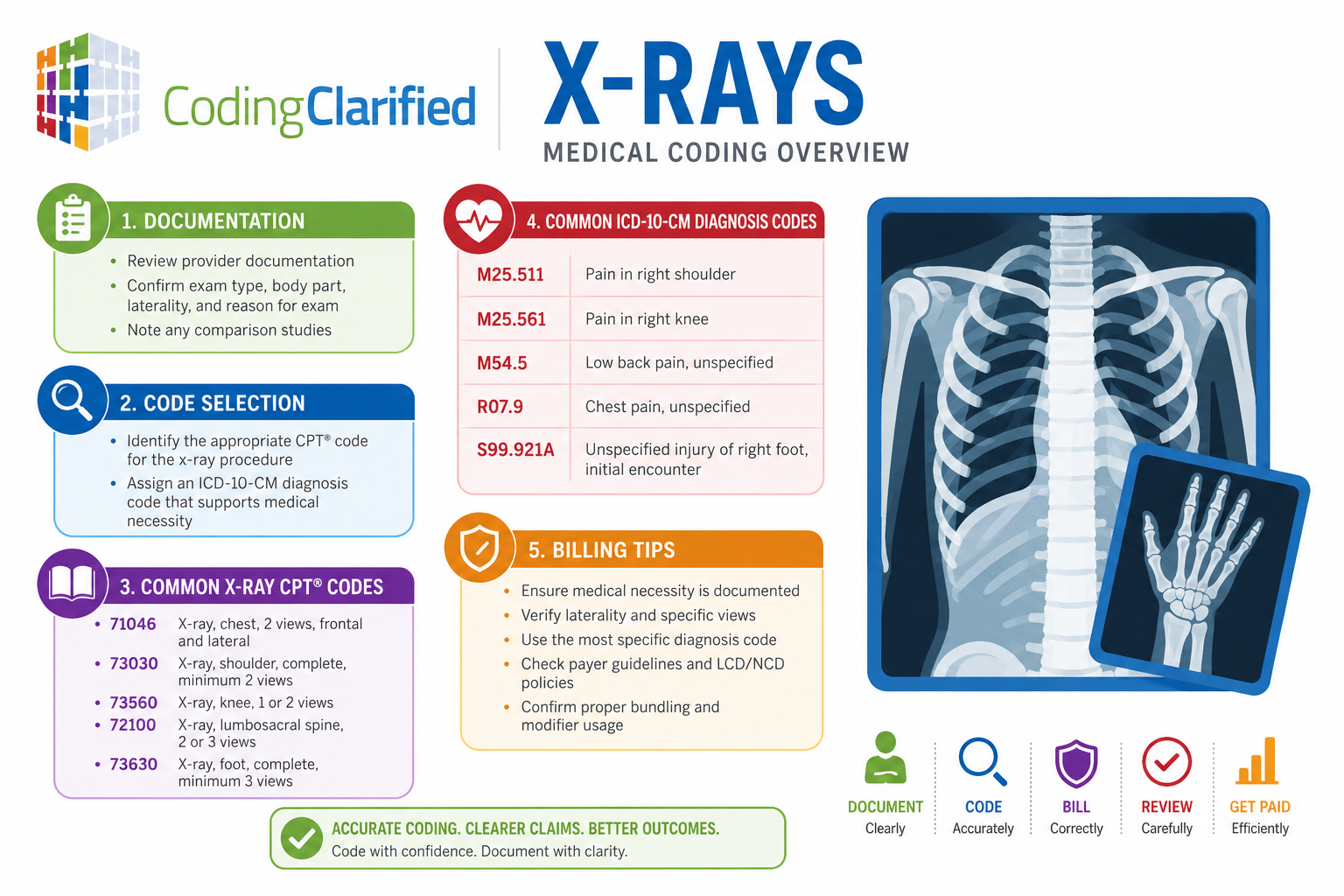
- X-ray procedures are reported using CPT codes from the 70000 series.
- The number of views directly impacts code selection.
- Medical necessity must support every radiology service.
- Modifiers -26 and -TC identify professional and technical components.
- Documentation must include body part, laterality, views, findings, and interpretation.
- NCCI edits may bundle certain radiology services.
- Medicare and commercial payers increasingly audit radiology claims for compliance.
- CPC students should understand component billing, radiology terminology, and common modifier usage for exam success.
What Is X-Ray Medical Coding?
X-ray coding involves assigning CPT and ICD-10-CM codes to diagnostic radiology services performed to evaluate injuries, illnesses, abnormalities, or disease processes.
Healthcare providers use X-rays to diagnose conditions involving bones, joints, lungs, abdomen, spine, and many other anatomical structures. Therefore, selecting the correct procedure code requires careful review of physician documentation and radiology reports.
Furthermore, coders must verify that the diagnosis supports medical necessity according to payer guidelines.
Understanding X-Ray CPT Codes in 2026
Most diagnostic X-ray procedures fall within the CPT 70010-79999 radiology section. However, selecting the correct code involves more than simply identifying the body part examined. In addition, coders must review the number of views obtained, physician documentation, and any applicable payer requirements. Consequently, accurate code selection requires a thorough review of the entire medical record.
Generally, CPT code selection depends on:
- Anatomical location
- Number of views obtained
- Whether contrast was administered
- Type of imaging performed
- Documentation provided by the physician
Below are several commonly reported X-ray codes.
| Body Area | CPT Code | Description |
|---|---|---|
| Chest | 71045 | Chest X-ray, 1 view |
| Chest | 71046 | Chest X-ray, 2 views |
| Chest | 71047 | Chest X-ray, 3 views |
| Chest | 71048 | Chest X-ray, 4+ views |
| Abdomen | 74018 | Abdomen X-ray, 1 view |
| Abdomen | 74019 | Abdomen X-ray, 2 views |
| Abdomen | 74021 | Abdomen X-ray, 3+ views |
| Ankle | 73610 | Complete ankle X-ray, minimum 3 views |
| Foot | 73630 | Foot X-ray, minimum 3 views |
| Lumbar Spine | 72100 | Lumbar spine, 2 or 3 views |
| Lumbar Spine | 72110 | Lumbar spine, minimum 4 views |
| Knee | 73560 | Knee X-ray, 1 or 2 views |
| Knee | 73562 | Knee X-ray, 3 views |
| Knee | 73564 | Knee X-ray, 4 or more views |
2026 Coding Tip
Always verify the documented number of views before selecting a CPT code. Choosing the wrong view count remains one of the most common radiology coding errors.
ICD-10-CM Diagnosis Coding for X-Rays
An X-ray CPT code alone does not establish medical necessity. Instead, the diagnosis code must clearly support the reason the imaging study was performed. For example, symptoms such as chest pain, ankle pain, or low back pain frequently justify diagnostic imaging. Likewise, traumatic injuries often support medical necessity when documented appropriately.
Common diagnosis codes may include:
- R07.9 Chest pain, unspecified
- M25.571 Pain in right ankle
- M25.572 Pain in left ankle
- M54.50 Low back pain, unspecified
- R10.9 Unspecified abdominal pain
- S82.891A Other fracture of right lower leg, initial encounter
- M25.561 Pain in right knee
- M25.562 Pain in left knee
Additionally, injury codes often require seventh-character extensions for encounter type.
Always code to the highest level of specificity supported by documentation.
Essential Documentation Requirements for X-Ray Billing
Accurate documentation serves as the foundation for compliant radiology billing. Without proper documentation, even correctly assigned CPT codes may result in claim denials. Therefore, providers should document all required elements at the time of service. Additionally, complete records help support medical necessity during payer audits and appeals
To reduce denials and support reimbursement, medical records should include the following:
Medical Necessity
The provider must clearly document why the X-ray was ordered.
Examples include:
- Trauma
- Fracture evaluation
- Chronic pain
- Acute injury
- Respiratory symptoms
- Follow-up assessment
Body Part Examined
Documentation should identify the exact anatomical location.
Laterality
When applicable, records should specify:
- Right
- Left
- Bilateral
Number of Views
The radiology report must indicate the exact number of images obtained.
Interpretation and Report
A qualified physician or radiologist must provide a formal interpretation.
Without an interpretation report, providers generally cannot bill the professional component.
Ordering Provider Information
Documentation should identify the provider who requested the imaging study.
Global, Technical, and Professional Component Billing
One of the most important radiology concepts involves component billing.
Radiology services consist of two separate parts:
Technical Component
The technical component includes equipment, supplies, technologist services, and image production. In other words, this portion represents the resources used to obtain the images. Meanwhile, the professional component represents the physician’s work in reviewing and interpreting those images. Together, these components make up the global radiology service
- Equipment
- Supplies
- Technologist services
- Image production
Report with modifier -TC.
Professional Component
The professional component includes:
- Physician interpretation
- Report generation
- Medical decision-making
Report with modifier -26.
Global Service
When the same entity performs both components, bill the global CPT code without modifiers.
Example
A physician office performs an ankle X-ray and sends the images to an outside radiologist.
The physician office reports:
- 73610-TC
The radiologist reports:
- 73610-26
This ensures each party receives reimbursement only for its portion of the service.
Modifier Usage for X-Ray Coding
Proper modifier assignment significantly impacts reimbursement.
Common radiology modifiers include:
| Modifier | Description |
|---|---|
| -26 | Professional component |
| -TC | Technical component |
| -59 | Distinct procedural service |
| -RT | Right side |
| -LT | Left side |
| -76 | Repeat procedure by same physician |
| -77 | Repeat procedure by another physician |
However, coders should never append modifiers solely to bypass edits. Documentation must support every modifier used.
Medicare and Payer Guidelines for 2026
Medicare continues to emphasize medical necessity and documentation integrity. Consequently, providers should expect increased scrutiny of radiology claims. Furthermore, Medicare Administrative Contractors (MACs) may issue Local Coverage Determinations that affect reimbursement. For this reason, coders should routinely review payer policies and updates.
As a result, radiology claims frequently undergo review when documentation lacks sufficient detail.
Important Medicare Considerations
- Medical necessity must be documented.
- Diagnosis codes must support the imaging service.
- LCD policies may affect reimbursement.
- Documentation must support repeat imaging.
- Component billing must be reported correctly.
Moreover, Medicare Advantage plans may impose additional requirements beyond Original Medicare guidelines.
Always review payer-specific policies before claim submission.
NCCI Edits and Bundling Rules
The National Correct Coding Initiative (NCCI) helps prevent inappropriate unbundling of services. Accordingly, coders should review NCCI edits before submitting claims. Additionally, certain imaging services may be bundled into larger procedures. Therefore, modifier usage should always be supported by documentation rather than applied automatically.
Therefore, coders should routinely review NCCI edit tables before billing radiology services.
Common bundling situations include:
- Emergency department encounters
- Postoperative imaging
- Multiple imaging studies performed during the same visit
- Imaging performed during other procedures
In certain situations, modifier -59 may allow separate reimbursement when documentation supports distinct services.
Nevertheless, modifier -59 should only be used when medically necessary and appropriately documented.
Common X-Ray Coding Scenarios
Chest X-Ray for Persistent Cough
Patient presents with chronic cough.
Possible coding:
- CPT: 71046
- ICD-10-CM: R05.3
Right Ankle Injury After Fall
Patient presents with ankle pain following a fall.
Possible coding:
- CPT: 73610
- ICD-10-CM: M25.571
- Additional injury code if fracture is confirmed
Lumbar Spine Pain
Patient presents with chronic low back pain.
Possible coding:
- CPT: 72100
- ICD-10-CM: M54.50
Always review documentation before assigning final diagnosis codes.
Common Mistakes to Avoid
Even experienced coders make radiology coding errors. Nevertheless, many of these mistakes are entirely preventable. By contrast, organizations that implement regular audits often identify errors before claims are submitted. As a result, they experience fewer denials and improved reimbursement outcomes
Avoid these common mistakes:
- Selecting the wrong CPT code based on views
- Omitting modifier -26 or -TC
- Billing without a formal interpretation report
- Reporting duplicate technical and global services
- Failing to verify medical necessity
- Ignoring NCCI edits
- Using unspecified diagnosis codes when more specific codes exist
- Missing laterality documentation
Regular audits can identify these issues before they result in payer denials.
CPC Student Tips for Radiology Coding
Radiology questions appear regularly on the CPC exam. Therefore, students should dedicate sufficient study time to the radiology section. Additionally, understanding modifier usage can significantly improve exam performance. Most importantly, students should practice identifying the correct CPT code based on the documented number of views.
To improve your score:
Learn View Requirements
Many exam questions test the number of views required for specific codes.
Understand Component Billing
Know when to use:
- -26
- -TC
Review Radiology Guidelines
Pay close attention to CPT radiology section instructions.
Highlight Common Codes
Focus on frequently tested codes such as:
- 71045–71048
- 73560–73564
- 73600–73610
- 74018–74021
Practice Reading Reports
The CPC exam often includes documentation excerpts requiring accurate CPT selection.
Related Coding Clarified Articles
For additional coding guidance, review these related resources:
- Computed Tomography (CT) CPT Coding: The Ultimate Quick-Reference Guide (2026 Update)
- Evaluation and Management (E/M) Guidelines for 2026: The Complete Guide
- Medical Coding Foreign Body
- ICD-10 External Cause Codes for Medical Coding
- Emergency Dept Services
Find additional coding resources at:
Coding Clarified Medical Coding Blog
Authoritative Resources
For the most current coding guidance, review:
- AAPC Radiology Coding Resources
- CMS Medicare Coverage Database
- CMS National Correct Coding Initiative (NCCI) Policy Manual
- AMA CPT Resources
Frequently Asked Questions About X-Ray Coding and Billing
What CPT code series is used for X-rays?
Most X-ray procedures are reported using CPT codes from the 70000 radiology section, with code selection based on the body area and number of views obtained.
When should modifier -26 be used?
Modifier -26 identifies the professional component when a physician only interprets the X-ray and provides the report.
When should modifier -TC be used?
Modifier -TC identifies the technical component when a facility performs the imaging but does not provide the interpretation.
Can I bill an X-ray without a radiology report?
No. To bill the professional component, a documented interpretation and report must exist in the medical record.
Why do payers deny X-ray claims?
Common reasons include lack of medical necessity, incorrect diagnosis coding, missing documentation, incorrect modifier usage, and NCCI edit violations.
Does Medicare require medical necessity for X-rays?
Yes. Medicare requires documentation that clearly supports the reason for the imaging study and justifies the service performed.
Are X-rays bundled into other procedures?
Sometimes. NCCI edits may bundle radiology services with other procedures when they are considered incidental or part of a comprehensive service.
What is the most common X-ray coding mistake?
One of the most frequent errors involves choosing the wrong CPT code because the documented number of views does not match the code reported.
Final Thoughts
Accurate X-ray coding requires much more than selecting a CPT code. Coders must evaluate documentation, verify medical necessity, understand component billing, apply appropriate modifiers, and review NCCI edits. Furthermore, staying current with Medicare policies and payer requirements helps reduce denials and improve reimbursement.
As radiology audits continue to increase in 2026, organizations that prioritize documentation accuracy, coder education, and compliance reviews will be better positioned for long-term success.
Coding Clarified Blog Radiology https://codingclarified.com/medical-coding-radiology/