Vascular and Interventional Radiology (VIR) is one of the most detailed and guideline-driven areas of medical coding. These procedures involve minimally invasive, image-guided treatments performed by interventional radiologists using catheters, wires, stents, embolization materials, and other devices.
Because many VIR procedures involve multiple components—such as catheter placement, imaging supervision and interpretation, and therapeutic intervention—accurate coding requires careful attention to documentation, CPT guidelines, and bundling rules.
Understanding how these procedures are structured will help coders assign the correct codes and avoid common errors.
What Is Vascular & Interventional Radiology?
Vascular and Interventional Radiology uses imaging guidance such as:
-
Fluoroscopy
-
CT
-
Ultrasound
-
MRI
to diagnose and treat diseases through small incisions or catheter access.
Common procedures include:
-
Angiography
-
Angioplasty
-
Stent placement
-
Embolization
-
Thrombolysis
-
Venous access procedures
-
Dialysis access interventions
Because these procedures are often complex and involve multiple steps, coders must review the operative report carefully.
Key Coding Principles
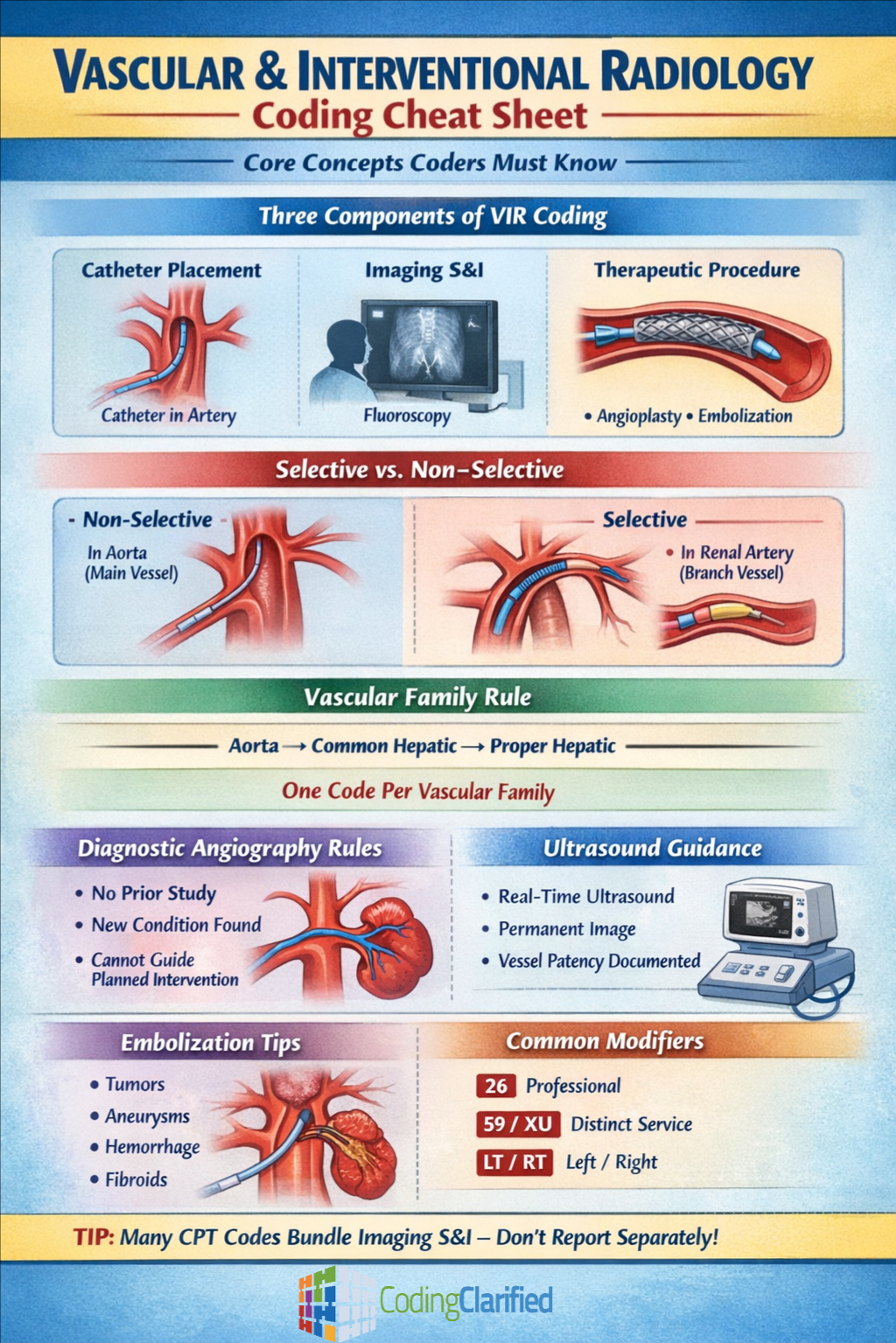
Understand the Three Components of VIR Coding
Many interventional radiology procedures include three coding components:
1. Catheter Placement
This represents where the catheter was advanced in the vascular system.
Examples include selective and non-selective catheterization.
2. Imaging Supervision and Interpretation (S&I)
These codes describe the radiologist’s interpretation of imaging used during the procedure.
3. Therapeutic Intervention
This is the actual treatment performed, such as angioplasty, stent placement, or embolization.
Important tip:
Many modern CPT codes already include imaging supervision and interpretation, so separate S&I coding is often not allowed.
Selective vs Non-Selective Catheterization
Correct catheter placement coding is critical in vascular procedures.
Non-Selective Catheterization
-
The catheter remains in the main vessel and is not advanced into branches.
Example
Catheter inserted into the abdominal aorta.
Selective Catheterization
-
The catheter is advanced into a specific branch vessel.
Examples include:
-
Renal artery
-
Hepatic artery
-
Superior mesenteric artery
The highest level of catheterization achieved is typically coded.
Coders must understand vascular anatomy to correctly assign these codes.
Vascular Family Rules
One of the most important concepts in interventional radiology coding is the vascular family rule.
A vascular family refers to all vessels that originate from the same primary artery.
Key guideline:
Only one selective catheterization code per vascular family is typically reported unless the catheter exits and reenters the family.
Example:
If a catheter is advanced from the aorta into the common hepatic artery and then into the proper hepatic artery, this is considered the same vascular family.
Only the highest level of selectivity is coded.
Bundled Imaging in Modern CPT Codes
Many interventional radiology CPT codes include imaging supervision and interpretation.
This means:
Do not separately report radiology S&I codes when the CPT code description already includes imaging guidance.
Example procedures that commonly include bundled imaging:
-
Angioplasty
-
Stent placement
-
Embolization
-
Thrombectomy
Coders should always review the CPT parenthetical notes and guidelines.
Diagnostic Angiography Rules
Diagnostic angiography may be coded separately when it meets certain criteria.
A diagnostic study is reportable when:
-
No prior diagnostic study exists
-
Prior imaging is inadequate
-
A new clinical condition is discovered
-
The diagnostic study leads to a decision for intervention
However, diagnostic angiography cannot be separately coded when it is performed solely to guide a planned intervention.
Documentation must clearly support medical necessity.
Access Site Coding
Access for vascular procedures is typically obtained through arteries or veins such as:
-
Femoral artery
-
Radial artery
-
Brachial artery
Access itself is generally included in catheterization codes and should not be coded separately unless a distinct procedure was performed.
For example:
Ultrasound guidance for vascular access may be separately reported if documentation includes:
-
Real-time ultrasound guidance
-
Permanent image recording
-
Documentation of vessel patency
Embolization Procedures
Embolization procedures are used to block blood flow to treat conditions such as:
-
Tumors
-
Aneurysms
-
Hemorrhage
-
Uterine fibroids
Coding depends on:
-
The vascular territory treated
-
The number of treatment sites
-
Whether multiple arteries were embolized
Careful review of documentation is necessary to determine whether multiple embolization codes are appropriate.
Modifier Use in Interventional Radiology
Modifiers are frequently required in vascular coding.
Common modifiers include:
Modifier 26
Professional component when only the physician’s interpretation is reported.
Modifier 59 or XU
Used to indicate distinct procedural services when allowed.
Modifier LT / RT
Used when procedures are performed on the left or right side.
Always verify modifier usage based on payer policies and National Correct Coding Initiative (NCCI) edits.
Documentation Tips for Accurate Coding
Accurate coding depends heavily on complete documentation.
Interventional radiology reports should include:
-
Access site
-
Catheter pathway
-
Vessels catheterized
-
Diagnostic findings
-
Interventions performed
-
Devices used (stents, coils, etc.)
-
Imaging guidance used
The operative report should clearly describe the vascular anatomy and procedural steps so coders can determine the correct CPT codes.
Common Coding Mistakes
Reporting multiple catheterization codes in the same vascular family
Only the highest level of catheterization is typically reported.
Separately coding bundled imaging
Many modern CPT codes already include imaging supervision and interpretation.
Coding diagnostic angiography without medical necessity
A diagnostic study must meet specific criteria to be separately reportable.
Ignoring vascular anatomy
Understanding arterial branches is essential for correct selective catheterization coding.
Final Thoughts
Vascular and Interventional Radiology coding requires strong knowledge of:
-
Vascular anatomy
-
CPT guidelines
-
Bundling rules
-
Documentation requirements
Because these procedures often involve multiple components, coders must carefully review operative reports and CPT instructions before assigning codes.
When coded correctly, interventional radiology procedures accurately reflect the complexity of the services performed and ensure proper reimbursement.
Understanding Radiology Medical Coding: Key Concepts and Practices